

A Lack Of Judgement
A Lack Of Judgement
Covid Series: Vaccines, part three

‘However beautiful the strategy, you should occasionally look at the results.’ Winston Churchill
We find ourselves living in interesting times, in the midst of a 'global pandemic' as the media likes to remind us and in order to 'save lives' and 'return to normal' we must take the vaccines, which have been helpfully designed and supplied in the blink of a cosmic eye. That was the message, is still the message, even if it is fraying around the edges somewhat.
The vaccines have been approved – well, not approved exactly – but they are safe and effective. Okay, they may not be unsafe and it depends on what you call effective. But, these minor quibbles aside, it's still essential that you take them, to demonstrate that you are a good citizen, to protect others, even if the vaccines can only be shown to protect you...maybe.
Nonetheless, government (or private corporations, the distinction having become a little blurred) want you to be able to wear your badge of honor, pour encourager les autres, so vaccine passports will be heading your way. It would only be right if a small incentive were offered, so flights, ball games, restaurants, life in general will be your reward. As for the unenlightened; they'll fall into line eventually.
Of course, there are two elements that must be satisfied, even for the most ardent admirer of the establishment; one, that there really is a clear and present danger and two, that vaccines are more likely to be the answer than not. In a functioning democracy, where journalists act as our proxies 'speaking truth to power', this could be a high bar to meet, even when the facts are undeniable. However, and even if we disagree as to the why, the what is obvious. In this case, the what is the fact that dissenting voices have been silenced, that the corporate media has spoken as one and the spirit of inquiry and necessary skepticism has been trashed.
Generally, this is not necessary if the facts speak for themselves. So, let's have a look at those two elements. Is there a clear and present danger, a public health emergency, currently? Was there one in December, when both the US and the Europe issued their authorizations? And are vaccines the only solution?
Ongoing pandemic?
In the US, the Secretary of Health and Human Services declared just such an emergency on 31st January, 2020; six days before the first US death was attributed to Covid.
Four days later, the same entity opened the door to vaccine trials by issuing a declaration under the PREP Act citation Public Readiness and Preparedness Act that provided liability immunity to drug companies for manufacture, testing, development and distribution of any drug that might be granted an Emergency Use Authorization (EUA), due to the fact that
'there is no adequate, approved and available alternative to the product for diagnosing, preventing or treating the disease or condition.' (1)
This would seem sensible, would it not? To authorize trials in potentially viable vaccines, which can be conducted in the background whilst the authorities are simultaneously battling the pandemic in the here and now and investigating any other, existing pharmaceutical products that might make experimental vaccines redundant. As a backstop - albeit an inherently risky one, given the near certainty that clinical trials would be truncated and an EUA rather than full approval would therefore be necessary – but still a possible option, in extremis. And, at the time, you could certainly argue that it was better to be safe than sorry and that it was possible that this was a genuine, deadly pandemic.
Implicit within the declaration is the idea that the public health emergency must still be in progress when a possible EUA is issued and contained within the definition of the EUA is the explicit corollary that there should be no alternative; it's this product or bust. Was this the case?
“By the time of consideration for approval of the vaccines, the health systems of most countries were no longer under imminent threat of being overwhelmed because a growing proportion of the world had already been infected and the worst of the pandemic had already abated. Consequently, we demand conclusive evidence that an actual emergency existed at the time of the EMA granting Conditional Marketing Authorisation to the manufacturers of all three vaccines, to justify their approval for use in humans by the EMA, purportedly because of such an emergency.”(2)
That letter was addressed to the European Medicines Agency by the Doctors for Covid Ethics, who number well over a hundred, all employed as experts in the field; currently. Bear in mind that authority to distribute the vaccines was granted in December, ten months after the initial declaration of a public health emergency. So, what were the numbers like then?
If you have faith in the figures with which you're presented, which would be touching, then case numbers, worldwide, were beginning to peak; from around 300,000 active cases per day for the summer months, by the end of November it was in excess of 600,000. Deaths, which had been at an average of 6,000 a day for six months, regardless of testing volume had also doubled, to 12,000 per day.
However, testing in western democracies had sky-rocketed over the same period. For example, the UK and the US were conducting seven times as many tests as they had in April and other countries were similarly zealous and yet positives had only risen by a factor of two. Further, deaths from respiratory diseases with symptoms indistinguishable from Covid typically increase dramatically in the winter months.
Given what we know of the deeply flawed methodology employed to record Covid deaths and the fact that influenza was allegedly down by an unprecedented 98% worldwide, a wise man might, at this juncture, find himself connecting some dots. He might also factor in the knowledge that increased testing seemed to be running up against the law of diminishing returns.
He might have remembered that science also existed before February 2020 and, as a result, taken salient advice on the known behaviors of viral pandemics. And having done all that, he might reasonably have concluded that the risk of an aggressive vaccination campaign with experimental drugs against a pandemic that wasn't what we had originally thought it was, was a step too far. That the risk far outweighed the possible rewards. But wise men have been in short supply, lately.
Only option?
This second leg of a EUA must also be satisfied. There needs to be no viable alternative, either as a prophylactic or as a cure. And the vaccines themselves have to be shown to be effective.
It was apparent from an early stage that other treatments were available and the evidence has been steadily stacking up ever since. Hydroxychloroquine, a venerable anti malarial treatment which has been in circulation as an approved medication for around sixty years, was shown to be very effective if taken in moderate doses, whilst a patient was in the early symptomatic stages of the disease.
Some studies found that symptoms were swiftly dispersed in two or three days in 80-90% of cases. Currently, there have been more than 200 studies, with over 350,000 patients; or, to put it another way, about four times as many patients as the vaccine trials, combined.(3) Not only that, but in moderate doses there are very few side effects and, as an off patent drug, treatments are very cheap.
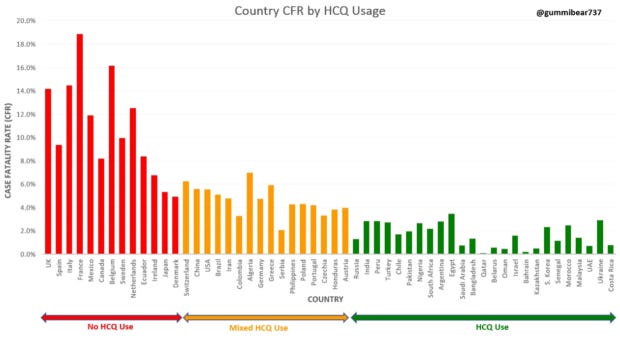
Figure 1 (4)
Some feel that hydroxychloroquine was doomed as soon as President Trump endorsed it. However, it is not the only non-patented treatment to suffer that fate; ivermectin, an anti-parasitic drug with an excellent safety record, was also championed, especially by front line doctors, as evidenced in Congressional hearings. Vitamin D, Zinc, even Vitamin C; the list of effective existing treatments with very little downside is long, but seemingly unconvincing to the grown-ups.
So, onto the vaccines, then. Were they demonstrated to be of use? As detailed in a previous article ('Here and now'), the evidence is less than convincing. Indeed, it would not be surprising if the vaccines were far less effective than claimed. It is clear from a detailed (40 page) petition to the FDA that a central pillar of the vaccine trials for both Moderna and Pfizer was wholly inadequate, relying as it did on the PCR test to record a positive or negative Covid test. This test, as detailed elsewhere ('Statistics, damn statistics') is not designed to perform the task of accurately recording live infection and, without that certainty, any trial results are deeply suspect.(5)
Decisions sometimes need to be taken in sub optimal conditions; things you'd like to know cannot be ascertained, the things you do know are inadequate in their scope and you don't know what it is you don't know. But when you have the best part of a year, essentially unlimited resources and a scientific treasure trove to plunder, you are in a better position than most. A well informed weighing of risk and reward should be a given, shouldn't it?
Results
This is where it gets difficult. It depends how you look at it and it depends what you are willing to believe. On 24th March 2021, in the US, the VAERS Adverse Reactions database was registering 3,964 deaths and 162,610 injuries due to the Covid vaccines, which seems like a lot when compared to other vaccines.(6)
And whilst the media is full of reports of elderly people producing vast numbers of antibodies after vaccination (e.g. Epoch Times, 14/10/21(7)), the data show that a third of people over 80 had no neutralising antibodies 17 days after vaccination. If you contrast this with the fact that only 1% of younger people found themselves in the same boat, you start to get the picture.(8)
This is not entirely surprising, given that immune response in the elderly has always been found to be sluggish. Whether this information had also extrapolated from the clinical trials is unknown. One could reasonably say, in an understated way, that this is a bit of a shame, seeing as how the group most at risk seem to be gaining no discernable benefit from vaccination.
British and Danish studies in nursing homes this year demonstrate that vaccinations caused a surge in infections and that residents and workers had a much higher risk of infection in the 10-14 days after vaccination.(9) Indeed, there were outbreaks in nursing homes all over Europe. Across Britain, deaths during the winter epidemic peaked almost five weeks after mass vaccination campaigns began in earnest. During a ten-day period in late January, Britain averaged more than 1,200 deaths per day.(10)
It surely doesn't take a Nobel Prize winner to work out that, if you vaccinate during an epidermic and the immune system reacts in the way that you intended (i.e. it is fully occupied in dealing with the consequences of the vaccination), a live virus challenge during this time might be problematic? You increase the risk still further by vaccinating residents who have already received a flu vaccination.
In other news, the AstraZeneca vaccine has been temporarily banned in numerous European countries, despite the European Medicines Agency trotting out its now familiar line about the benefits outweighing the risks. Denmark has even banned the vaccine permanently.
The issue appears to be that there have been undeniable clusters of deaths, in patients who are younger and in good health. The cause of death has been given as Thrombocytopenia, a very rare brain disorder resulting from a critically low blood platelet count. It seems the cases couldn't be ignored. It also seems that a vaccine that may result in a very low platelet count might affect more than just the brain.
In the US, the Johnson and Johnson vaccine has been temporarily suspended for similar reasons. It will be interesting to see how this is dealt with as the problem looks more like a class based problem, rather than being specific to a single vaccine. If that is found to be so, Pfizer and Moderna will also be dragged into the spotlight
Further, if it is found that the vaccine caused the problem and the authorities still reinstate the EUA, it is inevitable that further deaths will follow. It's one thing to claim an error of judgement at the outset of the enterprise, but quite another to ignore detrimental evidence during it and press the start button again.
What are the odds that adverse events, particularly connected to blood thinning or clotting, are much higher than reported? It's difficult to overlook rare occurrences, but heart attacks and strokes are much more commonplace and, potentially, easier to attribute to other causes. It's a racing certainty that the figures we are given are the absolute minimum.
As an example, VAERS has long enjoyed a reputation as a hideously inaccurate tool. It largely relies on self reporting and it has been reasonable to assume, in general terms, that perhaps 1% of adverse events make it onto the database. In this case, I doubt whether that degree of diminution would apply to deaths, but it may apply to the recording of other adverse events; especially if people are led to believe that some sort of reaction is normal.
As should be apparent by now, I don't believe that the criteria for an EUA was met. Some of the facts are clear and in the public domain, some are accessible if you dig enough while others are closely guarded secrets. It is also entirely possible that there is a deliberate policy to mislead us, in order to achieve the declared outcome, which is to vaccinate pretty much everyone. And then, probably, do it all again next year. With drugs that still aren't approved.
Certainly, at present, and even with state control of all the metrics, problems are still making themselves known. If two of the four main vaccines have been suspended, despite the best efforts of the authorities to convince us that there was nothing to worry about, we have big problems on our hands. This is not a place you find yourselves in when you exercise sound judgment.
Citations
https://www.gov.info.gov/content/pkg/FR-2020-03-17/pdf/2020-05484.pdf
Figure 1 https://beforeitsnews.com
https://childrenshealthdefence.org/wp-content/uploads/Dr.-Lee-Amended-Reply-Final.pdf
https://www.medrxiv.org/content/10.1101/2021.03.03.21251066v1.full
https://www.medrxiv.org/content/10.1101/2021.03.08.21252200v1
Berenson, Alex. Unreported Truths About Covid-19 and Lockdowns: Part 4: Vaccines (p. 26). Blue Deep, Inc.. Kindle Edition.