

Cannon Fodder

“It's difficult to get a man to understand something, when his job depends on him not understanding it.” Upton Sinclair
The alternative history of the Covid pandemic, if such a thing ever reaches the public consciousness, will be truly shocking, not the least for the callousness that will be front and center. It is one thing for the elites to scheme for power or profit, as so many people seem to have realized (and are willing to express in private conversation). It is quite another for that same elite to kill people, either by an overt act or by wilfully preventing treatment. And yet, that is what has happened and it has happened on an industrial scale. It tells us everything we need to know about how the people are viewed by those in charge.
I'm not talking about sending elderly patients with Covid back to their nursing homes, without informing them of their diagnosis, although that has happened in many locations. I'm talking about treatments that work which have been demonized and banned, as a result of which thousands of people have died unnecessarily. Not a few thousand, either. In all probability, hundreds of thousands.
The mantra was, from very early on, we have to wait for the vaccines. There was never any official enthusiasm for re-purposing drugs, apart from Donald Trump championing hydroxychloroquine (HCQ) Never any banner headlines, never any hope. You have been told that they are unsafe, that other drugs don't work. Once more:
“An Emergency Use Authorization (EUA).... may allow the use of unapproved medical products, or unapproved uses of approved medical products in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions when certain statutory criteria have been met, including that there are no adequate, approved, and available alternatives.”(1)
By that definition, there must be no viable alternatives. But there are. There are a number of drugs, and even vitamins, that work to combat Covid 19. For instance, there are numerous studies on the usefulness of humble Vitamin D in prevention or amelioration of Covid;
“Thus, the evidence seems strong enough that people and physicians can use or recommend vitamin D supplements to prevent or treat COVID-19 in light of their safety and wide therapeutic window.”(2)
“Vitamin D deficiency, which impedes good immune function, is common during winter and spring in regions of high latitude. There is good evidence that vitamin D deficiency contributes to the seasonal increase of virus infections of the respiratory tract, from the common cold to influenza….”(3)
Sound familiar? Ivermectin has many passionate supporters and shares a similar Covid journey as hydroxychloroquine (and azithromycin (AZ). I am going to concentrate on HCQ, with a side dish of Vitamin D, as proxies with which to lay bare the conduct of governments and health authorities across the globe.
Hydroxychloroquine was approved for use in 1955 as a treatment for malaria – it's also used to treat rheumatoid arthritis and lupus. It's not obscure – this recently maligned drug is on the World Health Organisation's 'List of Essential Medicines'. It's been used, safely, for 65 years and was available over the counter for pennies; until, that is, governments started to restrict its use. France converted it into a prescription only drug suspiciously early on in proceedings, on 15th January 2020 and other countries followed suit. And here's another interesting fact. By 2005, it was known that HCQ was a potent inhibitor of SARS, either as a prophylactic or in the early stages of disease.(4) You read that correctly.
At the outset of the pandemic, 300,000 people in the United States were already taking hydroxychloroquine (HCQ) and azithromycin (AZ). At least that many in the UK, also, as a treatment for rheumatoid arthritis.(5) And initially, physicians who actually treated patients with Covid 19 believed HCQ to be the most effective treatment (37%), with AZ coming in second (32%). A typical treatment protocol was 800mg prescribed on day one with 200-400mg for 4-5 days thereafter. Doctors didn't wait for Covid test results; they knew that early outpatient treatment was the key.(6)
After all, the alternative, which was employed by the vast majority of other doctors, was no treatment at all for high risk patients; come back when you're worse and we'll send you to hospital. So, naturally, the authorities decided that clinical trials had to be conducted, despite the fact that the drug was approved worldwide and was clearly working. There were two large scale trials – the Solidarity trial in the US and the Recovery trial in the UK.
Now, given the treatment protocol being followed by physicians, as stated above, what would you expect these trials to do? The idea would be to test the hypothesis in a controlled environment, would it not? No. Instead, hospitalized patients (not outpatients) were given 2.4g on day one and 800mg thereafter, three to four times the safe amount. These are toxic doses, given to patients who were already ill enough to be in hospital. The trials were designed in such a way that they tested neither of the parameters of real world prescription. And the trials weren't just botched; a large number of patients died. Why would anybody do that?
At the same time, in May 2020, one of the world's most prestigious medical and scientific journals, The Lancet, published an article purporting to show that HCQ treatment was associated with increased mortality. After a hail of criticism from medical professionals, it was discovered that the entire article was a lie and it was retracted two weeks later. But the damage was done – which must have been the entire point of it. France, Italy and Belgium immediately revoked HCQ authority and the WHO pressured other countries to do the same. The corporate media, who had fallen over each other to cover the publication of the article, predictably ignored the retraction. If you were actually interested in reporting the truth, that’s another puzzler.
Across Europe and the US, pressure was brought to bear on medical associations, on front-line physicians, on medical journals. Instead of being an over the counter medication, HCQ became a prescription drug and from there on in, state control was re-established. But out in the real world, there have been hundreds of studies demonstrating the curative powers of HCQ.(7)
“A reverse natural experiment happened in Switzerland. On May 27, the Swiss national government banned outpatient use of hydroxychloroquine for COVID-19. Around June 10, COVID-19 deaths increased four-fold and remained elevated. On June 11, the Swiss government revoked the ban, and on June 23 the death rate reverted to what it had been beforehand. People who die from COVID-19 live about three to five weeks from the start of symptoms, which makes the evidence of a causal relation in these experiments strong.” (8)
But in most of the western world, HCQ was dead and buried. Elsewhere, not so much…
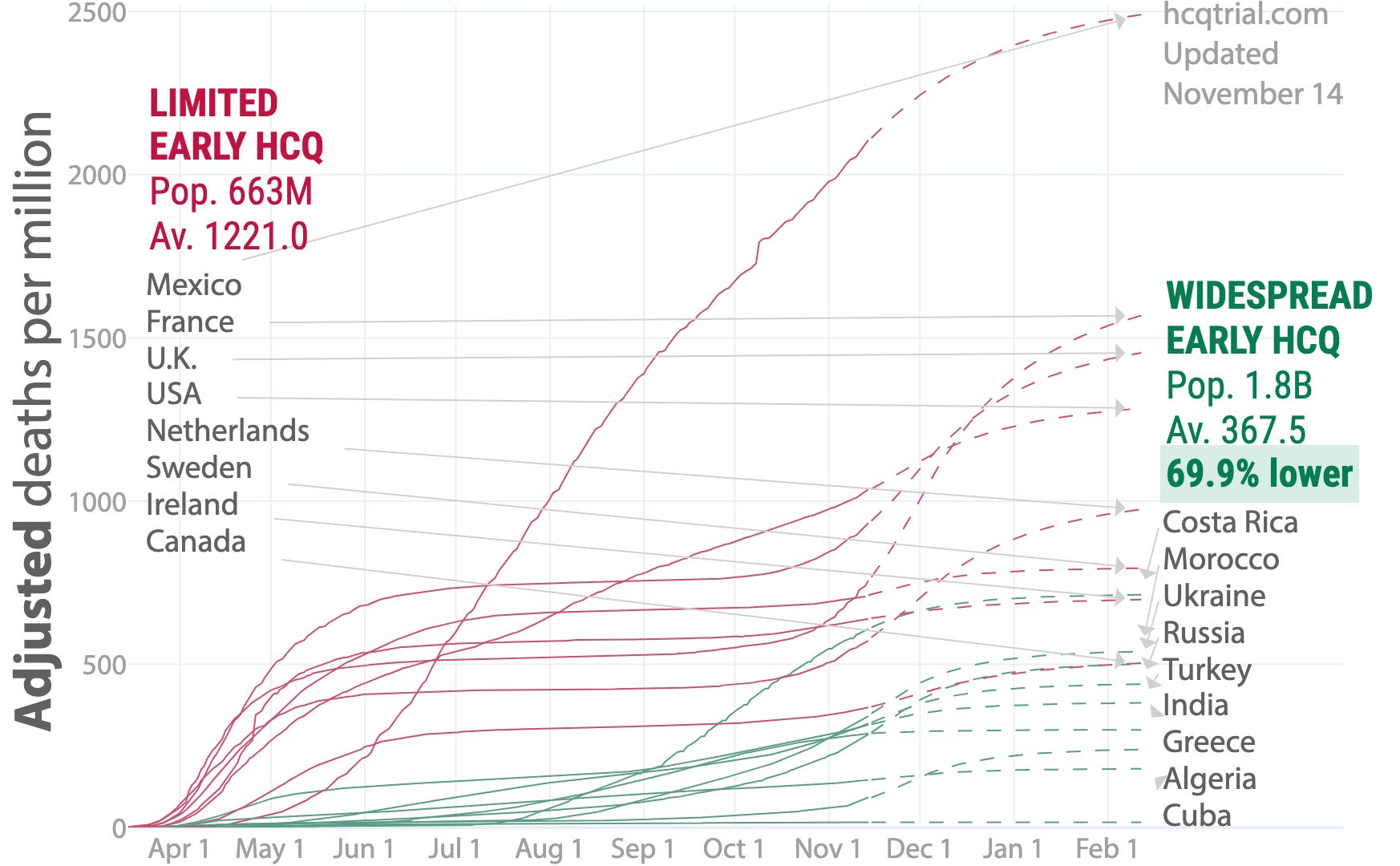
“Many countries either adopted or declined early treatment with HCQ, effectively forming a large trial with 1.8 billion people in the treatment group and 663 million in the control group. As of November 14, 2020, an average of 138.5 per million in the treatment group have died, and 588.4 per million in the control group, relative risk 0.235. After adjustments, treatment and control deaths become 267.8 per million and 889.8 per million, relative risk 0.30. The probability of an equal or lower relative risk occurring from random group assignments is 0.030. Accounting for predicted changes in spread, we estimate a relative risk of 0.30. The treatment group has a 69.9% lower death rate.” (9)
Strange things were happening. Even though HCQ was out, a drug called remdesvir was apparently okay to re-purpose as a treatment (without trials) , according to Dr Fauci of the National Institute of Health (NIH). This is a man who demands randomized trials for HCQ, but who refers to not yet approved remdesvir as the 'standard of care', despite evidence that is far less persuasive than that for HCQ.(10) I'm only speculating here, but is it possible that the fact that remdesvir is a patented drug got anything to do with it? Or that ten members of the NIH Board responsible for writing the Covid guidelines have a financial interest in the company that owns the patent, Gilead Science?(11)
Bear in mind that HCQ was the treatment of choice by physicians in the US and Europe during the early stages of the pandemic. At the end of March 2020, HCQ was being prescribed by 37% of physicians, with AZ the next most prescribed at 32%. This peaked in the next fortnight or so at around 56% in the US and 63% elsewhere. However, by 26th May (after the Lancet article) there had been a global decline in HCQ treatment, to 23% in the US and 41% elsewhere.(12) Coincidentally, remdesvir treatment was on the increase, from a lowly 12% in March, despite only showing mild effectiveness in hospitalized patients.(13)
So, had physicians realized the error of their ways, ignored prior science and voluntarily swapped treatment to a much more effective drug? Or had the CDC and NIH issuance of guidance that HCQ was not to be used for the treatment of Covid except in hospital, by which time it was much less effective, or during a clinical trial, the reason? Or, possibly, President Trump mentioning its effectiveness on March 23rd?(14)
Whichever reason you ascribe, there is blatant hypocrisy here and a chilling disregard for easily verifiable evidence. On the one hand, drugs, in use for fifty years with excellent safety records, shown to be effective in saving lives, can't be used because of the lack of clinical trials. On the other, experimental drugs, going through Phase III clinical trials (prior to being authorized) on hundreds of millions of people, which were only tested on mildly sick, generally healthy people and which do not stop disease transmission. One treatment was available from the beginning and worked, one took ten months to arrive and nobody can say what its impact will be.
And how would it have been ethically allowable for front line doctors, the ones actually treating patients, to conduct clinical trials in the midst of a pandemic, in order to justify using HCQ to the NIH? If one accepts that the only reason for wishing to prescribe hydroxychloroquine is because you believe it works and will stop patients becoming seriously ill and possibly dying, how do you only give it to half and give the rest a placebo or nothing at all? How does that square with the Hippocratic oath?
Isn't the entire purpose of clinical trials to test new drugs, to see if they are effective and to ensure there are no nasty side effects? So, when you have drugs (or vitamins), whose long term effects are known, which are proven to work in a real world situation, whether by accident or design, why would it be legitimate to refuse to countenance using them as treatments? What harm could come of it, especially when you have no viable alternative? There is only upside. Especially when you already know that HCQ helps in the treatment of SARS-CoV, a virus with a DNA sequence that is 80% identical to the virus known as SARS-CoV-2.
Some might say that it's inconsistent to advocate utilizing HCQ, AZ, ivermectin and the like, regardless of specific clinical trials for Covid, whilst excoriating the authorities for the vaccine experiment. But it's a pedantic debating point, at best. One set of drugs are safe, cheap, authorized and known to be effective. The others...the exact opposite, at present. And a process is only there to get you to your destination. If you have already arrived, there is no requirement to make the journey. Becoming a slave to the process is counterproductive and time consuming.
But, as a final test, let's just assume that the likes of the NIH and the WHO are right; all existing drugs are unsuitable, dangerous, whatever they want us to believe they are. They must be tested in trials. But we're still a year away from a vaccine and we don't have anything to counter the great plague. What about something completely uncontroversial, like Vitamin D? It couldn't hurt, could it?
“There is insufficient data to recommend for or against the use of Vitamin D for the prevention or treatment of Covid 19.”(15)
That's Dr Fauci's considered opinion and, to add insult to injury, nobody has bothered to update that advice since July 2020. Not exactly fulsome, is it? If you read that, you might think there was no point in taking it. The UK government, as late as December 2020, was still saying there was insufficient evidence that Vitamin D was helpful and, unoriginally, called for more trials. You would be entitled to ask why, after ten months, they were still unable to do anything other than sit on the fence when asked to give advice about a vitamin.
It's doubly puzzling when studies involving over 4,000 Covid patients show that Vitamin D deficiency that is not sufficiently treated is positively associated with COVID-19 risk.(16) So, there's long standing evidence that a deficiency of Vitamin D is associated with viral respiratory infections and specific evidence that it is also, predictably, a risk factor with Covid 19 but, despite that, government guidance is non-committal at best.
Is it as simple as no patent, no profit? There could be no prophylactic, no treatment because the vaccines could not have been authorized in that scenario? Does that provide enough motive for deliberately botched trials in which people died? Or could it be that the numbers of Covid 19 'cases' have been grossly inflated and treatment with HCQ would have exposed that deception, as it would have been ineffectual? Or is there another, more consuming reason?
Since May 2020, hundreds of thousands of people have allegedly died of Covid 19. HCQ, Vitamin D and other treatments have been denied the vast majority of those people. The overwhelming evidence of efficacy and safety has not just been ignored, it's been actively smeared and undermined. Organisations like the WHO, the NIH in the US and the European Medicines Agency have been the leading agencies in that effort. Given what are objective, provable facts, they have been complicit in the deaths of many thousands of people.
Citations
Mercola J, Grant WB, Wagner CL. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients. 2020;12(11):3361. Published 2020 Oct 31. doi:10.3390/nu12113361
Martin J Vincent, et al Chloroquine is a potent inhibitor of SARS coronavirus infection and spread Virology Journal 2005, 2:69 doi:10.1186/1743-422X-2-69
Dr Harvey Risch, Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients That Should Be Ramped Up Immediately as Key to the Pandemic Crisis Vol. 189, No. 11 DOI: 10.1093/aje/kwaa093 Advance Access publication: May 27, 2020
https://newsweek.com/key-defeating-covid-19-already-exists-we-need-to-start-using-it-opinion-1519535
https://hcqtrial.com
https://aapsonline.org/hydroxychloroquine-is-not-about-trump/
https://covid19treatmentguidelines.n.h.gov/panel-financial-disclosure/
Dr Harvey Risch, Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients That Should Be Ramped Up Immediately as Key to the Pandemic Crisis Vol. 189, No. 11 DOI: 10.1093/aje/kwaa093 Advance Access publication:May 27, 2020
as per (8)
https://covid19treatmentguidelines.nih.gov/supplements/vitamin-d/
https://medrvix.org/content/10.1101/2020.05.08.20095893vl.full.pdf