

Deadly Dispatch

I don't know about you, but one of the aspects of the 'vaccination' campaign has always gnawed at me – the problem reconciling the obvious damage that a pathogenic spike protein will do to the body with the appalling, but none the less sub-genocidal casualty figures. How can it be that some people suffer and yet some don't?
Before I delve into the detail; I know that looking into things that appear to weaken the case can be off-putting, especially when we are under relentless attack by all and sundry, or so it seems. The possibility that our investigation may end up offering succor to the enemy is not a welcoming one. The prosecutorial rule is never to ask questions you don't know the answer to. And it's also true that we are working off scraps here, relatively speaking. They know everything and we know what they tell us. However, while their public pronouncements, executive summaries and talking heads have stepping over the line from merely misleading to outright falsehoods, the published data frequently undermines them and it is to this we turn. And, actually, we want to know simply because we want to know and there is one other important use to which any knowledge can be put.
A couple of caveats. I do realize that it's early days and that we can expect to see an awful lot more damage as immune systems deplete and people succumb to infections that would never have previously troubled them. Plus, of course, the longer term damage from auto-immune diseases and the reactivation of dormant conditions. There are certainly issues with the physical accuracy of the jabber and how much of the ‘vaccine’ stays in the muscle, person to person. And I also acknowledge that people are not machines, that some will be more vulnerable than others due to age, weight, existing conditions and any number of variables that I am almost certainly ignorant of. But still...
It's not as if all those that survived the first few rounds of jabs only managed to do so by the skin of their teeth. We must all know people who had a bit of local soreness and that was pretty much it. Or the ones who had a fever for a day or two, but suffered naught after that. Again, so far. But, if you're reading this you are sufficiently clued up to know that there are thousands who have keeled over with cardiac issues in the first couple of days and others who have bled out due to their sudden lack of white blood cells, the result of the massive damage caused by the circulating pathogen and the clotting that follows in its path.

Figure 1
Easy to see why they don't want to count anyone as 'vaccinated' until 14 days post jab.
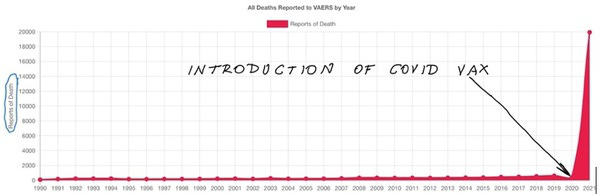
Figure 2
Those are just to establish the fact that we are not imagining things; that there is a smoking gun to be detected. And, as if that data aren't enough, there's more. The eagle-eyed among you will have spotted this already. It's one more example of an increasingly threadbare narrative coming apart at the seams. The CEO of OneAmerica, a health insurance provider of some repute – the company is worth $100 billion – spoke at an online news conference last week. Among his more illuminating comments was the following:
“We are seeing, right now, the highest death rates we have seen in the history of this business – not just at OneAmerica. The data is consistent across every player in that business.”(1)
This increase wasn't in older people; this was in the working age group, 18-64, and the increase in the third quarter of 2021 was 40%. To put that in context:
“Just to give you an idea of how bad that is, a three-sigma or a one-in-200-year catastrophe would be 10% increase over pre-pandemic.”(2)
And it wasn't just deaths – claims for short and long term disability were also exponentially higher. The death and injury peaks were confirmed by the head of the Indiana Hospital Association, too. Predictably, neither of them could think of any variable that might have impacted these figures, but at least they were raising a red flag. The beginnings of an answer wasn't too hard to come by:

Figure 3
But why Indiana? Does it have a particularly high 'vaccination' rate? No; it's 52% fully jabbed, which puts it in 43rd place out of 50 states (3) and well adrift of the 70% plus in the likes New York and New Jersey. But given that these totals are irrespective of population size, maybe it's just a big state. Well, the three states that surround it on the graph (Tennessee, Minnesota and Wisconsin) are of similar size, all of them being in the range between 5.7 million and 6.9 million (4) and their vaccine injury reports are at most around 50% of Indiana's, which are more in line with Pennsylvania (13 million). So, something else is responsible for the anomaly.
My first thought was that there must have been an issue with quality control and the Indiana had been the unfortunate victim of yet one more negligent discharge from Big Pharma. So, I went looking and stumbled across something a little bigger. It transpires that, across America (and there is no reason to think that this pattern isn't being repeated where you are, as I'll explain towards the end), all the damage is being done by a very small percentage of the lots distributed. Of course, that doesn't invalidate the contamination theory. But other factors almost certainly do. Because both Pfizer and Moderna have very similar profiles.
The following information is courtesy of the dailyexpose.uk website, link provided in the citations. The control sample used was that of the annual flu vaccine. And, once again, the numbers involved will be a huge underestimate, because the only dataset available is our old enemy, the VAERS system. With that in mind; last winter there were 494 lot numbers issued; 480 of them were not even linked to a single death and only one lot was implicated in as many as two. So, a remarkably consistent return. The total number of adverse events was low (1,608, or an average of 3 per lot), there were 73 hospitalisations and 15 deaths; in total. And the distribution of the lots also followed a discernible pattern – nearly half the lots were only sent to a single state (44%), 17% went to two states, 10% went to three and so on. Only 0.4% of the lots went to as many as 12 states.(5)
It's fair to say that the Covid 'vaccines' were a similar story in one sense; only a small percentage were the cause of all the problems. It's just that those problems were so much bigger:
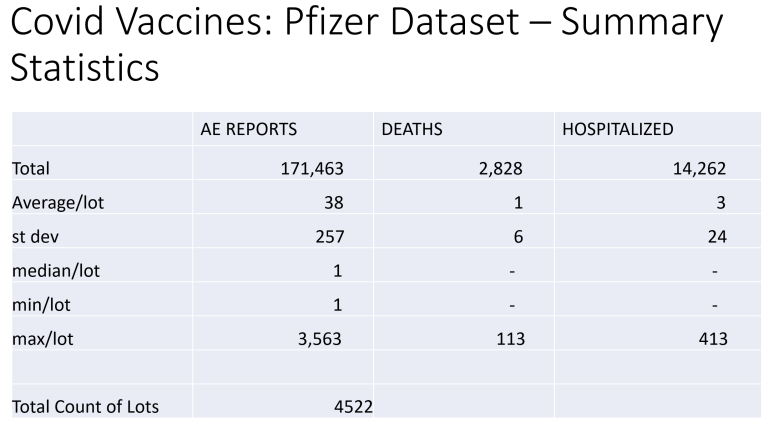
Figure 4
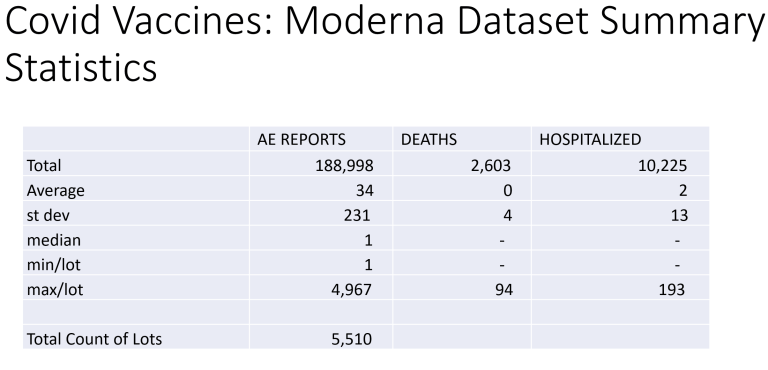
Figure 5
4% of Pfizer lots and 5% of Moderna's were responsible for all the deaths. All of them. 96% of Pfizer's and 95% of Moderna's didn't have a single death report attributed to them. Even more remarkably, 64% of Pfizer’s lots (2,908) didn't even have a single adverse event recorded against them. But Pfizer also had five lot numbers that returned between 61-80 deaths, five that had 81-100 deaths and two that registered over 100. It was a similar story with Moderna. So far, the contamination theory still holds water, although we might think it a little strange that both companies had the same issues in the same percentages. It's the next part that gives pause.
The distribution of the lots, when combined with the findings above, is where it's at:
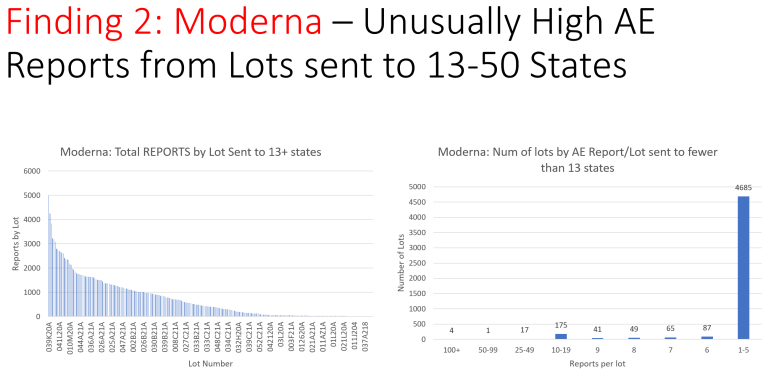
Figure 6
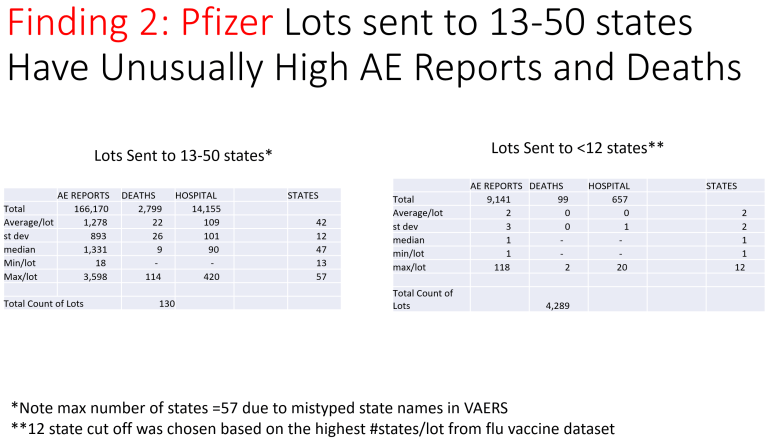
Figure 7
The problems came pretty much exclusively from lots that were widely distributed. In general, the lots were far more widely disbursed than those of the flu vaccines. Nonetheless, the pattern is startling and served to disguise the signal. The first question might be; why are the lots so widely distributed anyway? I'm assuming that neither Pfizer nor Moderna have a manufacturing facility in each state and that the lots are probably numbered in the order in which they are produced. It might be said that there was a need to distribute widely and equitably. The same could be said of the flu vaccines. And it still doesn't explain why the ones most dispersed are the most deadly. For example, only 130 of the more than 4,500 Pfizer lots were split between 13-50 states.
So what we end up with is the following. The vast majority of the 'vaccines' did not cause a single death; a good majority of them did not even attract an adverse event report. As an aside, that frequency is totally at odds with the clinical trial reports, when there were many more reports. But the 'vaccines' that did cause deaths were overwhelmingly from a small number of lots and these lots were also part of a very small number that were the most widely distributed. In the case of Pfizer, around 180 lots did all the damage. It just so happened that 130 of them went to more than 13 states and these were the ones that did. The Moderna story is very similar.
The net result is that the deadly batches were spread far and wide, wreaking havoc in a fairly uniform fashion and not attracting anywhere near as much attention as if an entire lot had landed in one location and devastated a community. And if we are to cling to the wreckage of the contamination theory, we must accept that these correlations are benign and that the outcome is mere coincidence. Granted, it doesn't fully explain the Indiana experience, but double the number of deaths than others is still less startling than many multiples of that.
If we perhaps lived in a world where Big Pharma had not already comprehensively fouled the nest, I might be inclined to contort myself into positions where I could posit a claim that although it walked like a duck, and quacked like a duck, it was in fact an aardvark. But Big Pharma is fresh out of credibility and it's difficult to look at this data and come up with an innocent explanation. It leads to other questions, of course. Like, what's in the other shots, for one?
Well, there are some clues, but nothing nailed on. The clinical trials are still ongoing for both Pfizer and Moderna. While Moderna only uses 100 microgrammes of mRNA per injection,(6) Pfizer/BioNTech has a plethora of options; 10, 20, 30 and 100 microgrammes in three different age ranges.(7) Is it possible that, with Pfizer at least, the vast majority of their 'vaccines' have been laced with very small doses of mRNA, less than they are letting on? That wouldn't explain Moderna, though.
There have been numerous press reports of 'accidental' saline shots instead of the jab in Minneapolis,(8) Ontario,(9) North Carolina,(10) South Carolina,(11) Miami,(12) Virginia (13)....the list goes on. That's a lot of mistakes; how does it even happen, given that the bottles are presumably labelled 'vaccine', not 'saline'? Don't expect an answer that bears scrutiny any time soon, unless you wish to place your faith in the 'fact checkers' online. Is it possible that these are just the instances that have come to light and that it points to the existence of unwitting control groups? After all, how would you know that you're being injected with saline in the first place?
The question is, of course, why? Why would some people be slated to suffer and possibly die and some not? It doesn't seem to be a strategy predicated on whether a state is blue or red; perhaps more data will color that assessment. Here, there can only be speculation. But I can see some sound tactical reasons for going this route; if the contamination theory is as hugely unlikely as it seems.
Too much death and injury too soon, and too contiguous could easily have seemed a tactical misstep. It would not only raise red flags almost instantly, despite the media running interference, it would also alienate the vast constituency of potential advocates. Anybody that has taken the 'vaccine' and suffered no ill effects can vouch for its safety and heap ignominy on the 'hesitant'. This, despite the fact that, even with this strategy, the number of injuries and deaths are still astronomical. But,as we have seen, that doesn’t alter the fact that there are still people who retain the ability to shut their eyes to the chaos around them and believe. Parsing the truly pathogenic 'vaccines' both numerically and geographically is sound. Not too much, too soon. And, even in the shots that caused no immediate harm, long term effects are unknown.
Big Pharma has form for traducing advocates:
““Patient Advocacy” groups have a unique power on Capitol Hill. They claim to represent the true voice of constituents, untainted by special interest bias. Politicians and the Food and Drug Administration use their endorsements as reflective of genuine public support.”(14)
When the FDA was obliged, by law, to hold discussions with these groups over the way drugs were approved, they were encouraged to take up several recommendations including giving greater weight to 'real world evidence' and 'patient reported outcome' in preference to time consuming and costly clinical trials. Even the reader with the more hopeful outlook on the substance of human nature might question why potential patients were arguing for less safety controls, rather than more. Such a reader would be disappointed to learn that:
“the vast majority of the groups the FDA included in the discussions—at least 39 out of 42, or 93 percent—have received funding from drug companies...
more than a third of the groups—15 that POGO has documented—have executives, directors, or other personnel from pharmaceutical or biotech companies on their governing boards.”(15)
Is this sort of behavior truly a surprise? Especially when the FDA is, effectively, a captured agency? I don't think so.
The strategy so far has been sound. But it's still difficult to hide all those injuries and deaths and not everybody can be told what to say at press conferences. Spreading the worst of it around hides the signal for longer, but not forever. And it doesn't change the fact that the jab should have pretty much the same effect on all of us. And it clearly isn't. Indiana seems to have found itself unwittingly on the front line.
Citations
(2) Ditto
(4) https://www.census.gov/library/stories/state-by-state.html
(6) https://www.clinicaltrials.gov/ct2/show/NCT04470427
(10) https://nypost.com/2021/04/19/walgreens-store-injected-saline-instead-of-covid-19-vaccine/
(12) https://www.miamiherald.com/news/coronavirus/article250779019.html
(13) https://www.newsobserver.com/news/coronavirus/article249846668.html
(14) https://theintercept.com/2016/12/01/new-report-exposes-patient-advocacy-groups-as-a-big-pharma-scam/
Figure 1

Figure 2 Ditto
Figure 3 CDC
Figure 4 https://dailyexpose.uk/2021/12/16/how-bad-is-my-covid-19-vaccine-batch/
Figure 5 Ditto
Retinoic Acid as a Vaccine Adjuvant Enhances CD8+ T Cell Response and Mucosal Protection from Viral Challenge https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3147979/
https://clinicaltrials.gov/ct2/show/NCT04353180
Assessment the Activity Value of Isotretinoin (13- Cis-Retinoic Acid) in the Treatment of COVID-19 (Isotretinoin in Treatment of COVID-19) (Randomized) (Isotretinoin)
https://clinicaltrials.gov/ct2/show/NCT04730895
Investigating the Role of 13cis Retinoic Acid in the Treatment of COVID-19 and Enhancement of Its Spike Protein Based Vaccine Efficacy and Safety. (Isotretinoin)
https://clinicaltrials.gov/ct2/show/NCT04396067
Aerosol Combination Therapy of All-trans Retinoic Acid and Isotretinoin as A Novel Treatment for Inducing Neutralizing Antibodies in COVID -19 Infected Patients Better Than Vaccine: An Innovative Treatment (Antibodies)