

Experimental Gene Therapies
Experimental Gene Therapies
Covid Series: Vaccine Update I

“No amount of evidence will ever persuade an idiot." - Mark Twain
'Vaccines'?
But, we have to try. And so, to one of the most contentious subjects of our time; vaccines and the artificial divide created by those using the 'pro' and 'anti' vax labels, as if it is impossible to be in favor of some and against others, which may be where a sizeable minority find themselves, incidentally.
A reasoned argument might go something like this; first show me the need, the inability of nature to overcome the disease without our intervention. Next, show me how it is, on balance, beneficial to society at large and then, finally, demonstrate that the remedy won't do more harm than good, won't remove one problem only to replace it with another. I might even want to use this to illustrate my position:
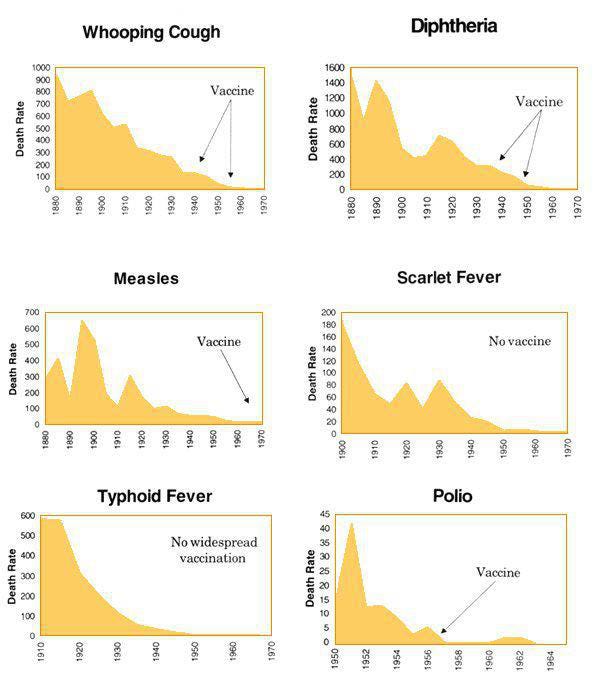
Figure 1: heartcom.org
Or this:
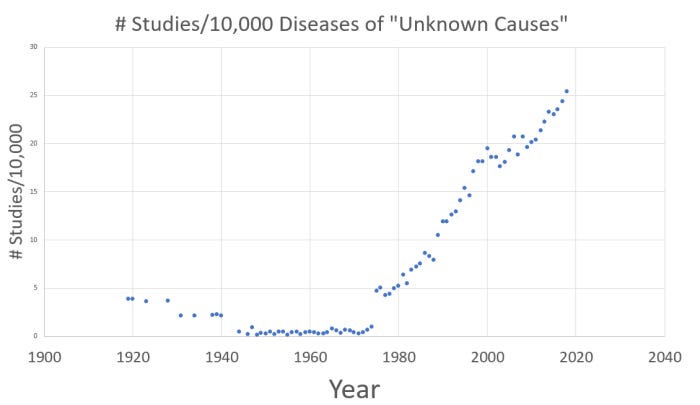
Figure 2: lewrockwell.com
Regrettably, the pro vaccine crowd (at least, the Big Media version) don't do reasoned argument; binary choices and shouty, ad hominem attacks are more their speed. Activists have changed the rules of this game, much as they have in most other areas of public life, to the extent that even people who have a case to make against the Covid jabs feel obliged to preface their remarks with phrases like “ I'm not anti vax (insert story about how they've vaccinated all their kids or similar), but...”.
Sadly, in today's pantomime, you are either for or against; no nuance is allowed. Actual evidence is increasingly irrelevant. As has been obvious for decades in the global warming debate, faith and vehemence are the attributes most representative of activists. It is becoming increasingly apparent that personality is the dominant factor in any belief system; a topic for another day.
To turn to the Covid 'vaccines', specifically, and bearing in mind that this is an update, not a rehash, not every aspect of the vaccine argument will be presented here. It is, however, worth revisiting the subject of whether the jabs are, in fact, vaccines. Firstly, any product that is still undergoing trials, whose effectiveness has not been evaluated is not, by definition, a vaccine. After all, establishing whether it works in preventing disease is the purpose of said trial; unless and until it is proved effective, it can only ever be an experimental treatment and referring to it as a vaccine is deliberately misleading.
Further, a treatment that does not a) prevent disease in the vaccinated and b) prevent them spreading the disease to the unvaccinated, or indeed to other vaccinated people, does not fit the definition of a vaccine. Unless the definition is changed, of course, which is already being attempted.(1) None of the main 'vaccine' suppliers make any claims to the contrary. Vaccines prevent infection and transmission – these treatments were not designed to do either.
In fact, if we were to proceed on the basis that the vaccines are actually targeting a condition known as Covid (see Real or Imagined?) they are the archetypal 'leaky' vaccine – a term that applies to an inoculation that isn't actually a vaccine, even if it is referred to as such, but is instead a treatment which enable symptoms to be ameliorated without killing the disease. If it were a vaccine it would, by definition, not be leaky.(2)
There are some serious risks associated with leaky vaccines; they allow a disease to mutate without actually being eradicated. Evolution being what it is, this can lead to more infective and deadly variants, as these can survive in a host who is vaccinated. Eventually, the disease (which was originally non lethal) mutates into a deadly pathogen, fatal for all unvaccinated hosts. This is what has happened with Marek's Disease in chickens. This would presuppose, of course, that there is in fact a virus to inoculate against.
They are, instead, experimental gene therapies. This should not be regarded as a partisan statement; it should not put one on the margins of the debate. It's a factual statement. The injection contains mRNA, material which instructs the host body to produce a foreign substance, a pathogenic spike protein. As such, it is hijacking our genetic structure. Were anyone able to question the drug companies, they would have no option but to confirm it, as the technology has been around for decades; in pharmaceutical circles, this is common knowledge. However, the Federal Drug Agency and the EU equivalent are not allowed to authorize experimental gene therapies, so they call them vaccines instead.
Okay, so they are a gene therapy. But they're not experimental, they're authorized for use, aren’t they? As so often, language is important; for the likes of you and me, so that we may understand the truth. For Big Pharma and the state, so that they may use words to confuse and mislead us. It all comes down to the difference between two words; authorized and approved. The truth is that no regulatory authority has approved these therapies for use. These treatments are authorized using a device called an Emergency Use Authority (EUA), because without it, the state thinks we'd all be dead in our beds – allegedly. So, the normal process of clinical trials was interrupted and, with our lives hanging in the balance, the state allowed Big Pharma to stick a needle in our arm and save us. Gratitude is in order.
Importantly, the EUA hasn't actually stopped the clinical trials; it's just that we are now the trial, whether we like it or not. The drug companies will still need to gain official approval in the end. Indeed, technically, the EUA could be rescinded at any moment, if our elders and betters determine that there is no longer an emergency, and Pfizer and Moderna would have to return to overt Phase III trials. Doesn't seem likely, does it? Not least because it would reveal that we have been enrolled in a clinical trial without our informed consent.
I would imagine that this interpretation of events may be novel to you, but only by virtue of it being buried by what passes for Big Media. Think about it – if a treatment is not yet approved but it is being administered, it must still be in trials. The drug companies themselves talk about seeking approval in 2022 or 2023; by admitting as much, they are telling you that trials are still ongoing. Even if there was a cohort of people still in a signed up, controlled clinical trial (which there isn't, except for specific subsets of the population such as transplant patients), we would still be in a parallel trial. Unless the rules for clinical trials are going to be rewritten or, better yet, ignored, which is the current strategy.
Clinical trials
Officially, the clinical trials were abandoned after a couple of months of what the drug companies were referring to as Phase III. As is well known, after laboratory testing in cell lines, animal testing is supposed to be next, followed by a number of phases where the product is to be refined and then refined further. You would ordinarily get to the end of animal testing in 3-6 years. This is because there are a variety of treatments being tested – various amounts of the 'vaccine', possibly different fillers (adjuvants), various treatment protocols – including the number and timing of them – and so forth. It is a process of discovery, all designed to establish which combination (if any) is safe and effective, not just in the short term, but in the long term too. The bar is set high, in theory at least; the vaccine has to be safe, necessary and more effective than anything else in nature or in a pharmacy.
In order for these trials to be completed, there are also control groups; those participants that get a placebo, rather than the treatment. To obviate both the well documented mental side of disease treatment – the placebo effect - and the tendency of scientists to give the game away to participants, the best studies are double blind – neither the human guinea pigs in the trial nor the front line researchers know who is getting what. Over time, the best version of the vaccine will be identified and, as that happens, more and more people are enrolled in the trials in order to test the product rigorously. It's not unusual for the whole process to take ten years; a large number never even make it as far as human trials.
So, that's what should happen. With the Covid ‘vaccines’, we are to believe that the trials were two months into Phase III when the EUA was granted; so, around ten months. And that everything had been done to ensure they were 'safe' and 'effective', the two buzzwords that are repeated, ad nauseum. There seems to be a cognitive issue here; if the 'vaccines' are safe and effective, and that was accomplished in ten months, why does it normally take 6-10 years? Surely, we should save time (and lives) by streamlining the process so that other drugs can come to market in similar time frames?
Alternatively, the FDA, European Medical Agency and others could admit the obvious, which is that they have been rushed through and issued under an Emergency Authorization and it is therefore possible, probable even, that there are side effects that can't yet be known, but the balance of risk and reward still favors the vaccines, in their judgement; even if the vaccines aren't necessarily safe any more and, as we shall see, certainly aren't effective. However, built into this risk/reward judgement should be the knowledge that the 'vaccines' aren't designed to act like vaccines and infection and transmission are not curtailed. This knowledge ought to mean that a severely circumscribed level of risk should be accepted if the potential reward is so negligible.
Instead, predictably, they want to have it both ways. To tell us that the reward is worth the risk, without giving any detail as to why they believe that (with growing evidence to the contrary), and that the vaccines are safe and effective because of the rigorous testing process that was never completed. Both these statements cannot be true and I would refer you, once again, to the word 'emergency'. The whole point is that, in an emergency, we should be prepared to take more of a gamble in order to succeed. Given that there is no evidence of excess deaths worldwide or even in the US over the course of 2020, despite the siren calls of Big Media, we can add 'emergency', 'safe' and 'effective' to the list of words that have been re-defined, joining the likes of 'vaccine' and 'isolated'.
Additionally, whilst animal trials were conducted, they were seriously curtailed and run at the same time as early human trials; and they were not a resounding success. Details are sketchy, but we know that they were abandoned in the autumn of 2020, if not why they were. Senate hearings in Texas have heard evidence that some of the animals died.(3) I need hardly point out that, whether successful or catastrophic, running these trials concurrently with human trials is unethical and pointless. The entire purpose of animal trials is to eliminate as much danger as possible before moving onto human trials.
“And there's the appearance that there was manipulation of safety data analysis and reporting in the Phase 1, 2, 3 clinical trials for some of these products by focusing on patients who had completed the study per protocol, as opposed to those that entered the study as intended to treat.
That's a subtle distinction, but what it means is that if you've only accepted one dose of vaccine under those clinical trial protocols and you have an adverse event, and you decide to drop it out, or they gently suggest that you shouldn't take the second dose, that information about the adverse events that you received — which would have made you at even higher risk for the second dose — is lost. It's not included in the safety analysis.
This is a classic way to manipulate safety data in clinical research, and it's strictly forbidden.”(5)
So, where exactly are we now? What phase of trials? And whose definition are we going to go by? The time honored one or a new one, re-imagined by the drug companies? We must still be in trials; the documents lodged by Pfizer, for instance, give a start date of 29th April 2020, a primary completion date of 2nd November 2021 and a study completion date of 2nd May, 2023.(4) They also list at least 18 different treatment protocols, some of them labelled 'boosters'. Bear in mind that this document has been amended several times since, including an amendment to include boosters for the 'South African variant'. If the original clinical trials were, in fact, completed, there has been plenty of opportunity to amend the dates. The NIH issued a press release on 27th July 2020, stating that the Moderna Phase III clinical trials were about to begin.(6)
Some questions naturally present themselves:
Is it the case that we are all Phase III participants, subject to these protocols of different doses, placebos etc without our knowledge? Even those of us who won't have the jab?
Is that why some people suffer adverse events and some don't?
Is there a placebo control group?
Are they tracking everything, doses, injuries, deaths? Surely, they must be if we are still in trials?
There have been numerous press reports of 'accidental' saline shots instead of the jab in Minneapolis,(7) Ontario,(8) North Carolina,(9) South Carolina,(10) Miami,(11) Virginia (12)....the list goes on. That's a lot of mistakes; how does it even happen, given that the bottles are presumably labelled 'vaccine', not 'saline'? Don't expect an answer that bears scrutiny any time soon, unless you wish to place your faith in the 'fact checkers' online. Is it possible that these are just the instances that have come to light and that it points to the existence of unwitting control groups? After all, how would you know that you're being injected with saline in the first place?
And how are the drug companies going to provide clinical trial data to the FDA when they come to seek authority in 2022/23? Are they going to limit it to the data they gathered before the EUA was offered and ignore over two years worth of real world injections in hundreds of millions of people? What should have happened is clear; we should have been afforded the same protections as clinical trial participants, which includes explicit informed consent (which can only be given if a full disclosure of known effects is given), medical monitoring, follow ups and so forth. Clearly, none of that has happened and it is not a discussion that has been allowed to take place in the public square.
We do know something though:
“Among the most critical tests, which must be performed prior to testing any drug or vaccines in a human being, is whether it can cause mutations in the DNA (genotoxicity), or whether it could cause problems with cells or tissues of the reproductive tract – including ovaries (reproductive toxicity). In the case of the Pfizer COVID mRNA vaccine ... standard studies designed to assess these risks were not performed in compliance with accepted empirical research standards. Furthermore, in key studies designed to test whether the vaccine remains near the injection site or travels throughout the body, Pfizer did not even use the commercial vaccine (BNT162b2) but instead relied on a “surrogate” mRNA producing the luciferase protein.”(13)(14)
Or, in other words, if they didn't do basic stuff, is it wise to credit them with doing detailed stuff? Another topic that has excited no curiosity is the subject of what is actually in the jab. I'm tempted to say that this is staggering; after all, even though so much of the detail of the Covid saga has not been aired, even the most ill informed must know that these 'vaccines' are using a new technique, never previously tried in humans and they must also know that they were developed quickly. Operation Warp Speed; the clue's in the name. Sadly, the lack of openness by the state and sheep like qualities of our fellow citizens are no longer a surprise. Nonetheless, what do we know about 'vaccine' ingredients?
Ingredients
The story, for public consumption, is that the 'vaccine' contains mRNA of just a small part of the virus, the spike protein. So, rather than getting the virus in the jab, like traditional vaccines, you'll only get that bit. The effect will be to make your body produce antibodies to the spike protein, so that if the real virus comes along, your immune system will recognize it and zap it. Simples.
Except, of course, it isn't. Unless you start asking questions, you might assume that the spike protein mRNA was the genuine article or, in other words, a small part of the actual virus. That, after all, is the inference. But no viral isolates were available when the vaccines were produced for the initial clinical trials (a situation that hasn't improved in eighteen months – go figure), so it's a synthetic spike protein instead. That fact alone should give pause for thought. It's not natural and yet it's going in your body, to combat something that allegedly is natural. There's more.
The problem with mRNA, if you're Pfizer or Moderna, is that Nature has decreed that it should be fragile, ephemeral. It can be destroyed if it is breathed on; that's where it fits into the grand scheme of things, for perfectly valid evolutionary reasons. But, if you're a drug company with billions invested in research into how to manipulate it, there is a need to make it more robust and that can only be done by artificial means. So, the synthetic spike protein is much more tenacious than anything found in Nature. It will stay active much longer (how much longer, nobody yet knows), performing its set task, which is to hijack the body's proteins to produce more versions of itself, in the hope that antibodies will be produced in response.
But further manipulation is required. The mRNA needs to be delivered into the cells which, as it stands, won't happen because the immune system is programmed to destroy any foreign RNA or DNA that it recognizes in the body. So, there needs to be another process which is capable of tricking the body into accepting the mRNA into its cells. This involves the creation of what's known as lipid nano-particles (which are coated with compounds), which encase the spike protein and which the body thinks are fats or oils, structures it doesn't recognize as a threat. Et voila; the spike protein is in like Flint. There are also other ingredients that have been added to the shot, which enhance the potency of the treatment; these are known as adjuvants.
There are some important factors to note, not directly connected to a discussion of the ingredients themselves, but rather their effect. A traditional vaccine injects a foreign viral fragment into the body in quantities anemic enough to produce antibodies without disease. The body only has that one task. These 'vaccines' require the body to perform two tasks, instead; production of the spike protein (artificial spike protein, remember?) and the antibodies to the spike protein. This will become important when we turn to the subject of injuries.
In the meantime, an inquisitive soul might ask the following questions:
What's in the synthetic spike protein that makes it different from the 'natural' one?
What are these lipid nano-particles coated with to get them though the cell wall?
What other adjuvants are in the shot? What do they do?
This is where information becomes sketchy, which is not what you would ordinarily expect, but which is becoming an all too familiar characteristic of the 'vaccine' saga.
It transpires that AstraZeneca uses the 'wild' spike protein; or what might be more usefully referred to as the sequence posted online by the Chinese, as there is still no isolated spike protein or virus shown to be infective and transmissable (see Real or Imagined). The others use a slightly modified spike protein which allegedly has the advantage of being a more efficient binder to human cells. This also reduces the number of non-neutralizing antibodies created – non neutralizing have a tendency to float around and cause havoc.(15)
However, as already mentioned, this spike protein is encapsulated in a lipid nano-particle in order to allow it to survive attack by the immune system and in order to trick the cells into allowing entrance. As an aside, doesn't that sound exactly like the sort of thing scientists do because they can? Without becoming too fundamentalist, we can probably agree that the human body, for most of us, is a miracle of construction. At a minimum, I would hope that anyone thinking of designing a procedure that involves deceiving the immune system would be asking themselves whether it was necessary, whether existing immunity wasn't enough and also, crucially, what the trade off might be both short and long term.
On the other hand, it might be exciting to just do it because you can and see what happens, which would be a more accurate description of the current state of affairs. One of the reasons why this is so is revealed when we take a closer look at what these lipid nano-particles, these shells around the spike protein, are composed of.
There are four ingredients; cholesterol, a phospholipid, an ionizable lipid and a PEGylated lipid. Without getting into the weeds too far, the first two are fatty lipids that cells like and the third possesses a positive charge to penetrate the cell. It's the last one that we are interested in.
When tracked via the specific scientific name, typically a combination of words and numbers, the Moderna version of this lipid is made by a company in China called Sinopeg.
The patent, also registered in China, clearly references the use of polyethylene glycol (the PEG part) and graphene oxide in coronavirus vaccines.(16) And Sinopeg list the nano-particles used in Covid 19 vaccines along with an explanation, which is now severely curtailed, but which wasn't prior to the discovery of their role. One of the ingredients of the polyethylene glycol lipids is graphene, which is, apparently, “ the thinnest, strongest and stiffest material ...an excellent heat and electric conductor”.(17)
This seems confusing at first, as graphene oxide is not included in the list of ingredients either on the fact sheets in the US or UK, nor in the filings for Phase III with the FDA.(18)(19)(20)(21)(22)(23) Why? Because it's a trade secret and trade secrets get a pass when it comes to public disclosure in patent applications. You or I might think that the whole point of a patent application is precisely that: to establish rights to trade secrets and transparency should, therefore, be expected. Otherwise, surely, the published patent (if granted) cannot actually be relied upon to tell the full story. Every other ingredient (as far as we know) is listed, but not graphene oxide. One can deduce from this, that no other constituent of the 'vaccine' is regarded as worthy of being kept secret. So, why would graphene oxide fit the mould?
Graphene is, indeed, an excellent conductor of electricity if it has a positive charge (it is currently neutral in the 'vaccine'), but it will annihilate anything it comes into contact with in those circumstances. It would need to be activated by an electro magnetic field. If this could be accomplished, it would create a problem; the only question would be the severity of it. And that, presumably, would depend upon the quantity of infected cells and their location. Additionally,
“...several typical mechanisms underlying GFN (graphene family nanomaterials) toxicity have been revealed, for instance, physical destruction, oxidative stress, DNA damage, inflammatory response, apoptosis, autophagy, and necrosis.”(24)
The presence of graphene oxide shouldn't be a surprise, to anybody familiar with the field of drug delivery. Research has been ongoing for years, especially as it pertains to hydro-gels.
“Graphene and graphene derivatives (e.g., graphene oxide (GO)) have been incorporated into hydro-gels to improve the properties (e.g., mechanical strength) of conventional hydro-gels and/or develop new functions (e.g., electrical conductivity and drug loading/delivery).” (25)
So, what of it? It's been studied for years and it's in hydro-gels, whatever they are. It must be okay. Well, you might think so. But it was only isolated in around 2004 and it seems that researchers have been so carried away with its positive qualities that they have largely neglected to test for downsides. However, one study made some rather obvious connections.
“...a team of biologists, engineers and material scientists at Brown University examined graphene’s potential toxicity in human cells. They found that the jagged edges of graphene nanoparticles, super sharp and super strong, easily pierced through cell membranes in human lung, skin and immune cells, suggesting the potential to do serious damage in humans and other animals.”(26)(27)
A further warning sign, if one were needed, would be the fact that the aforementioned hydro-gels are being researched by the likes of the Defense Advanced Research Projects Agency (DARPA) and Bill Gates. Indeed, a Silicon Valley company called Profusa, backed by both of the above, has developed a biosensor chip that is implanted under the skin using hydro-gel. It is marketed as an early warning system for Covid (28), but it does a lot more than that, including transmitting biological information over the internet. As I write this, it seems the stuff of conspiracy theorists, maligned and marginalized though they are.
Here's a Profusa press release from March 19th 2018:
“Today scientists are presenting results showing tiny biosensors that become one with the body…and stream data to a mobile phone and to the cloud….tiny biosensors composed of a tissue-like hydrogel, similar to a soft contact lens, that are painlessly placed under the skin with a single injection.”(29)
Doesn't seem so far fetched now, does it? At the time of writing, the FDA doesn't appear to have approved this yet, but given the involvement of DARPA, it would seem that an authorization is in the offing. Further, any testing or trials that may have been done have not been conducted in public, but as the rules on clinical trials seem to have become somewhat flexible lately, I wonder whether there's another EUA in the offing, possibly for use with booster shots?
The sensor is the size of a grain of rice and intended to be a permanent addition, as it will bind to the tissue around it. As altruistic as all this sounds, can we spot any potential for malpractice? Presumably, as well as signalling Big Brother that we have a slight temperature, it will also let the state know where we are; there's not much point in going to all that trouble to halt a pandemic in its tracks, if the carrier can't be located.
And there wouldn't be much point in locating the plague infested deplorable if there was no way to ensure he is quarantined. Can we detect any possible means of malfeasance? A temptation to fiddle the data, so that certain individuals guilty of “wrong-think” are pinged; perhaps repeatedly? Is it possible that we are witnessing a tiny example of overreach? Maybe it's just me. But it seems that yesterday's conspiracy theory is today's reality.
Interregnum
So far, I have set out what new information about the composition of the vaccines has come to light in the past couple of months, which is a considerable quantity, despite the combined efforts of that unholy trinity of government, Big Media and Big Pharma to memory hole it.
In particular, the presence of graphene oxide, a discovery made in early June by an analysis of an AstraZeneca phial,(30) but since identified in the Moderna and Pfizer 'vaccines' (by chemical designation). The 'fact checkers' have been busy online, framing a question they like the look of and answering it, rather than challenging themselves with the straightforward question of how a compound known to be damaging to both human and animal cells has found its way into a 'vaccine' and been authorised. Big Media have largely ignored it, as is their wont when facts get in the way of the narrative.
So, what do we know of the physical effects of the shots? Are we being kept fully abreast of events (you may wish to guess the answer to that one ahead of time)? And what conclusions can we draw?
Citations
Robert Malone https://articles.mercola.com/sites/articles/archive/2021/08/01/covid-vaccine-bioethics-concerns.aspx?ui=c6dab1d9f793d9702b5a6173bbaf0de1320ab79209c23435823c043e6a65fa7c&sd=20210418&cid_source=dnl&cid_medium=email&cid_content=art1HL&cid=20210801_HL2&mid=DM945487&rid=1223036418
https://nypost.com/2021/04/19/walgreens-store-injected-saline-instead-of-covid-19-vaccine/
https://www.miamiherald.com/news/coronavirus/article250779019.html
https://www.newsobserver.com/news/coronavirus/article249846668.html
https://www.docdroid.net/xq0Z8B0/pfizer-report-japanese-government-pdf#page=8
https://dearpandemic.org/spike-protein-differences-between-different-vaccines/
https://www.gov.uk/government/publications/regulatory-approval-of-covid-19-vaccine-moderna
https://clinicaltrials.gov/ct2/show/study/NCT04368728?term=immunogenicity+covid+tolerability+healthy&cntry=US&draw=2&rank=3
Ou et al. Particle and Fibre Toxicology (2016) 13:57 DOI 10.1186/s12989-016-0168-y
https://newatlas.com/graphene-bad-for-environment-toxic-for-humans/31851/
https://www.mddionline.com/implants/early-warning-system-detecting-infections-being-studied
Prof Dr Pablo Campra Madrid, Interim Report, Graphene Oxide Detection in Aqueous Suspension Observational Study in Optical and Electron Microscopy, Universidad de Almeira, Spain