

Next Level Gaslighting

What is it about Covid that we actually know for sure? For that matter, how can we identify how to know anything for sure? Which sources can we trust? How can we go about validating information? Over the past four years, my views on all of the above have undergone a degree of evolution; not by a huge amount, as an implicit trust of official sources was a condition of which I had already been cured. And, also, some sources which were moderately trustworthy in the early days of the 'pandemic', soon changed their tune when their data started to be used by the resistance. As time passed, even data that was previously impervious to corruption – such as absolute mortality statistics – were manipulated (usually by simply delaying updates by up to a year) and needed to be treated with care.
Fortunately, there is such a cornucopia of information that is routinely pumped out by a wide variety of entities that censoring it all is a non-starter and, in any event, would draw too much unwanted attention. There's also the Wayback Machine, the patent office, historic health data, statutorily required statistics, parliamentary and congressional records and so forth (the entrenched bureaucracy, beloved of the pencil pushing administrative state) and so the state's response has been to manipulate what they can, hide what they can (usually information that we don't even now exists), delay release of data they can't legitimately avoid making public, redact as much as they can away with and then ignore what they can't explain away, in the full and certain knowledge that the media has their back.
There are three primary sources of information and one secondary, but only two of the primary sources are worth a candle and, even then, they must be corroborated with other evidence until a picture starts to emerge. The secondary source is that of opinion articles, which are liberally laced with primary source material, but might also be somewhat slanted. The primary sources are quasi-official data (even though they've done their best to clean house), academic papers and first hand, anecdotal accounts from trusted sources.
Academic papers can no longer be taken at face value and the term 'peer review' is completely worthless. Those who have been paying attention know that science went bad a long time ago, well before the press followed suit. According to the science, opium, cocaine and tobacco were all harmless, at worst, and a positive boon, at best. The tobacco industry's scientific disinformation campaign was effective for five full decades.(1) Electric shock therapy, insulin shock therapy, epileptic fit theory, lobotomies, eugenics, SSRIs and opioid treatments are just a few of the missteps that the medical profession has made, all of which have been legitimized by 'the literature'.
All a Big Pharma or Big Government funded scientist needs to do these days is to write a paper that parses the available evidence (or makes some up out of whole cloth) in a way that supports the prevailing orthodoxy, get some of his or her mates – also funded by those same entities – to 'review' said paper and then publish it in scientific journals who (wait for it) are feeding at the same trough as all the other links in the chain. That science, as a whole, is terminally corrupted, is now publicly acknowledged.(2)
Official data, on the other hand, is not yet completely beyond the pale. Yes, it should be treated with caution, but attempts to manipulate it are often undone by other official data that is contradictory and, as previously mentioned, it's not always easy to erase the record. By way of example, the following two charts show the hospital demand for both fentanyl and midazolam in New York City in March/April 2020; both drugs are used when patients are intubated. Incidentally, note the blue line too, which represents a constant number of actual patients, not a huge surge.

Figure 1

Figure 2
And the simultaneous precipitous decline, across the entire country, in outpatient prescriptions for antibiotics.
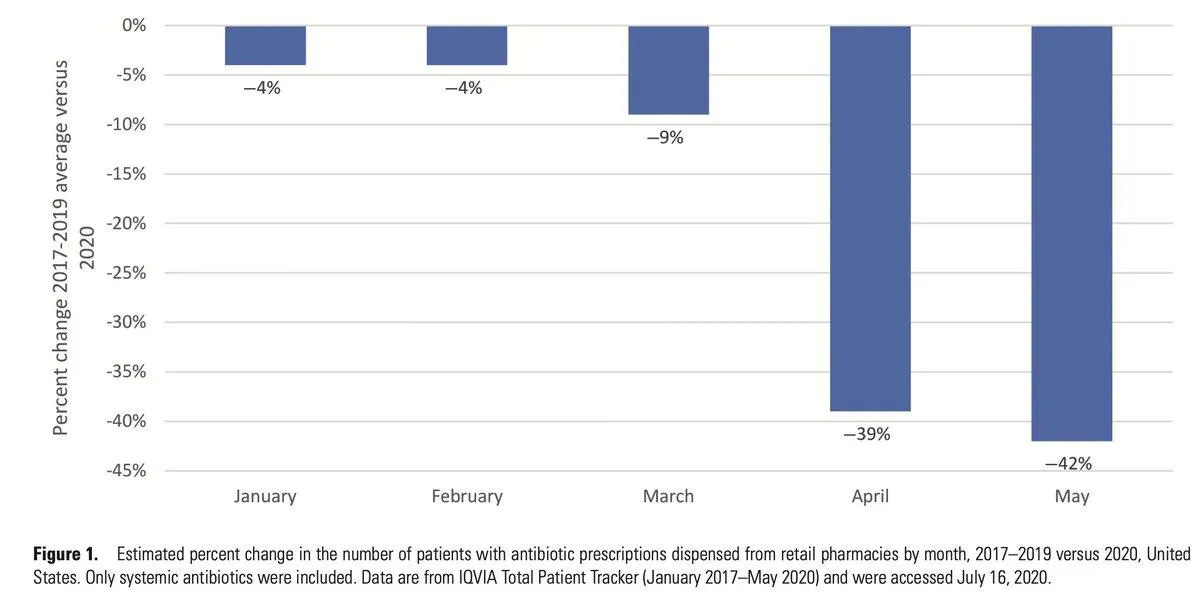
Figure 3
Primary sources such as these are used by legitimate actors to calculate trends, which then produce conclusions that can also be reached by the reader, because the original data is available. We are not being force-fed an evidence-free narrative. Anecdotal evidence from knowledgeable persons who have broken with the narrative – and have therefore been targeted as a result – should also be weighed in the balance. There are times when data alone cannot give the fullest of pictures. I acknowledge that subjectivity must still have a role, as calculating the authenticity of a source is still, in part, a matter of judgement. The hope is that, over time, that judgement will become much better informed.
And so, back to Covid. If we utilize the methodology as outlined above, what do we actually know for sure? I don't mean what we have reflexively understood to be fact over the past four years. Instead, let's strip it back to the absolute basics. Do we know that SARS-COV-2 actually exists? The answer? No, we don't, because we cannot implicitly trust those that tell us that it does and, if we assess our actual knowledge anew, we haven't been presented with unassailable evidence as to its existence. No scientific entity has provided evidence of isolation of the virus.
What we have are lines of genetic code that have been typed into a database and a 'disease' that, symptomatically, is identical to other respiratory diseases such as influenza and bacterial pneumonia; lines of code that were uploaded onto the National Institute of Health (NIH) genetic database on 28th December 2019 by a researcher based in Beijing and then removed on 16th January 2021.
Allegedly, the sample from which the code (which was incomplete) was obtained was that of a 65 year old, critically ill deliveryman.(3) However, none of that information can be relied upon; firstly, because this is the same China that faked photographs of Covid victims lying in the streets and, secondly, because we are being given this information by government, the same entity that has continually gaslit us about the 'pandemic' in general.
In addition, the PCR test was (is) less than useless as false positive rates of 90% plus were commonplace (depending on the cycle rate – sensitivity – of any particular batch of tests) and we have no way of knowing what the swabs were actually testing for, if anything. So, the 'cases' or positive tests are not evidence of anything, because we do not have access to any of the data that would prove that, in this instance at least, the state was truthful.
The distribution of the supposedly infectious disease also makes no sense, whatsoever. This is its prevalence in the United States, over two months after its alleged emergence.

Figure 4
How can that be possible? How is it only deadly in very limited locales? Likewise, how is it that the same virus that is supposed to have have killed 1.3 million poor and disabled Americans...
“...did not cross the more-than-thousand-kilometer land border with Canada, despite continuous and intense economic exchanges. Likewise, the presumed virus that caused synchronous mortality hotspots in March-April-May 2020 (such as in New York, Madrid region, London, Stockholm, and northern Italy) did not spread beyond those hotspots.”(4)
Further, how can we evidence the reality of asymptomatic spread? Especially as the entire concept is predicated on two assumptions; firstly, that Covid, as an infectious disease, actually exists and, secondly, (even if we set that first assumption aside), that a person who tested 'positive' for Covid actually had Covid, given the demonstrably unserviceable mode of testing? As it is, the allegedly asymptomatic only infected other family members 0.7% of the time, with whatever it was that the test picked up.(5) Or, they didn't infect anyone, either because they didn't have a disease that is non-existent, or because the test picked up the DNA of some other material that was simply present in the family member.
If SARS-COV-2 doesn't, in fact, exist; or, alternatively, if SARS-COV-2 does exist, but not in the form of an infectious disease, then the 'pandemic' narrative, already largely discredited in terms of the efficacy of the measures imposed in order to allegedly combat the disease, collapses entirely. And the evidence showing that there was no pandemic is comprehensive; contrastingly, the evidence (in the public domain) that demonstrates that Covid does exist in some limited form is anecdotal, but still compelling. It just isn't indicative of a pandemic-level event.
Covid allegedly struck right at the end of the infectious season cycle, which is unprecedented at that scale and it erupted simultaneously across different continents, immediately following the WHO declaration, but only in specific locations.(6) This is not how pandemics operate; they spread outwards from an initial source. Even allowing for the enhanced capacity for spread created by modern-day air travel, the timing is completely off. In addition, excess mortality repeatedly refused to cross state or national borders.(7)
Historically,
“...whereas epidemics of fatal infections are very real in care homes, in hospitals, and with degenerate living conditions, the viral respiratory pandemic risk promoted by the USA-led “pandemic response” industry is not a thing. It is most likely fabricated and maintained for ulterior motives, other than saving humanity.... Otherwise, in a stable society, mortality is extremely robust and is not subject to large rapid changes. There is no empirical evidence that large changes in mortality can be induced by sudden appearances of new pathogens.”(8)
Year-to-year winter-burden mortality is seasonal and remarkably consistent, peaking in the winter months, likely the result of the changes in seasonal humidity and its consequent effect on the ability of airborne pathogens to circulate.(9) In simple terms, heavy air inactivates pathogen-carrying droplets much more swiftly than dry air; hence, winter is a more co-operative disease partner than summer. Additionally, shortfalls in vitamin D and the prevalence of hormone-induced SAD (Seasonal Affective Disorder) render individuals even more susceptible to infection. However, the Covid peak only lasted a month, occurred at the wrong time of year, was absent in many places (for example, 34 of the 50 US states show no peak) and varies greatly in magnitude.(10) These are all contra-indicators. Ergo, it was not a pandemic.

Figure 5

Figure 6
Instead, it was a short-term, synchronized event; the excess deaths were the result of medical ‘blunders’. That is what the evidence is demonstrating. These types of peaks, as shown in Figures 5 and 6, are what we see at the other locations that were targeted. There was no widespread pandemic. There was the impression of one, which was created by the universal use of a PCR test that was configured in such a manner as to return a positive test from a wide variety of samples, including a quail, a papaya fruit and a goat.(11) But there is no evidence of contagion beyond this deception.
I appreciate that this might be something of a revelation, but that's what the data show. I'm reasonably confident that if the blob had information that would, in fact, demonstrate that there was a pandemic, they would be most anxious to share it with us. But they can't, because there obviously isn't any. But, somehow, peaks were nonetheless created; relatively large numbers of people died over the period of a month in spring 2020. How so? There are several factors in play.
Sending elderly patients who were suffering from a respiratory disease back to their care homes from hospital is one major factor, especially in New York, in the UK and in Sweden. That was a circumstance that could have easily been avoided, but was, instead, embraced. Then there is the curious case of sudden, near universal medical misdiagnoses.
For reasons that the medical profession has yet to elucidate, in March/April 2000 every inpatient with a respiratory disease was believed to be suffering from the new, novel coronavirus. Not any of the other (until that point) prevalent and treatable diseases that had been staples for decades, notably bacterial pneumonia:
“Pneumonia symptoms overlap heavily with SARS-CoV-2 symptoms and given the edict that antibiotics do not help in the treatment of SARS-CoV-2, it is inevitable that many patients suffering from pneumonia would have been denied antibiotics until it was too late for them to have a material effect.”(12)
Although 72% of US patients that were intubated were apparently given antibiotics, it would appear that they were not administered at the correct time or in the correct doses. We know this because of what was, effectively, an against-guidance control experiment in Europe:
“...physicians in Toledo, Spain, empirically administered antibiotics to covid-19 patients during spring 2020, contrary to official guidance. This resulted in zero hospitalizations or deaths in their care homes after they started routine administration. Their resulting mortality over spring 2020 was approx. 7% versus 28% in other comparable care homes (and the 7% died before they started routine antibiotic use).”(13)
A Romanian physical took a similar path, providing cheap medications and the antibiotic clarithromycin. She reported an unblemished record, with over 1,000 patients healed. In contrast, the intubation and oxygen therapy that was the default programme for the excess mortality hot-spots was a disaster. Intubation for lengthy periods can lead to cerebral edema and death. It is also known to promote bacterial pneumonia. This accumulated knowledge did nothing to ameliorate the Pavlovian response in the US, UK and Europe in March/April. Apparently, bacterial infections (and all other infections) suddenly all-but disappeared.

Figure 7
“The reduction in bacterial infections can only be attributed to changes in diagnostic testing, treatment and case definitions.”(14)
I suppose that it's conceivable that hospital staff were deceived; that they were seduced by the newfangled PCR test, which sent them off down a diagnostic dead-end, from which they returned, blinking into the light, a month later. Perhaps somebody, somewhere realized that they were in the midst of a pinpoint pandemic and that pretty much the only deaths were in care homes and hospitals in specific locations, and therefore changed tack. Perhaps.
However, the UK National Health Service's sudden deployment of widespread Do Not Resuscitate notices, culling the disabled and the infirm, often without permission or notification (in breach of the law), does not encourage the adoption of benign explanations for medical 'mistakes'.(15) Between 2nd March and 12th June 2020, there were 28,186 excess deaths in care homes in England alone, a 46% increase on the rolling average.(16) One is left with the distinct impression that a significant number of 'useless eaters' had been intentionally dispatched. The care homes of New York were similarly decimated, as were others throughout Europe.(17)(18)
But it's also possible that there was a limited release of a (non-infectious) pathogen in a few locales – this is where the anecdotal evidence comes into its own. Dr Pierre Kory, subsequently a notable advocate for ivermectin treatment, was on the front lines in New York and, unless we are to discard his testimony as partial or tainted (and I can't come up with a reason for doing so), it seems highly probable that some other mechanism was in play.
He details symptoms and a disease progression that don't easily square with other diagnoses; micro clotting, very high rates of loss of smell and/or taste, organizing pneumonia (not associated with bacterial infection), 'happy hypoxia' – patients were not struggling to breathe, despite very low levels of blood oxygen saturation – and dry lungs. At these later stages of infection, antibiotics had no effect. He came to realize that early intervention with antivirals were the answer.(19)
Dr Kory is an experienced doctor and he wasn't the only clinician who reported similar findings. He was convinced that he was witnessing a novel infection, but this disease was clearly confined to a small number of jurisdictions. It doesn't seem likely that it was infectious to any great degree, or it would surely have been more geographically pervasive. Nonetheless, even if we accept Kory's evidence, the spike in excess mortality was still only four weeks in length. It is certainly possible that other limited releases have also been effected since, but even those who believe they have contracted Covid at some point are still reliant on the blob for an explanation of what that is supposed to feel like.
Quite how such a disease might have circulated is unknown, although there are several suggestions – vapes tampered with, aerosols released or a contaminated water supply might be possibilities. The same uncertainty surrounds possible origins, because the only entities able to answer those questions are those who can no longer be trusted. Lines of code on a database are now potentially meaningless – how can we possibly know whether they relate to a genuine pathogen, or whether they are yet another deception?
But, if there was no pandemic; if, whatever it was that Kory bore witness to was simply a local phenomenon that failed to launch (or which was never designed to launch), what are we make of the 'variants'? How can there be variants, if there was no original virus? Because if there never was an infectious pathogen, there was never a disease that could mutate and produce variants.
The possibility that the entire variant narrative is false may seem like a step too far. However, once again, how do we know that they exist? Because the authorities tell us so? Because of a test that doesn't work? The symptoms associated with said variants are indistinguishable from other respiratory diseases – colds, RSV, influenza (which is, itself, simply an umbrella term) and others. How can we be sure that they exist? I can't see how we can.
I can see how pretending they do serves a purpose; it gives a rationale for boosters, fills the coffers of the 'vaccine' companies and keeps the specter of Covid in our peripheral vision. It normalizes the whole concept of pandemics, helps us forget that (with the exception of other beta tests earlier this century) pandemics are incredibly rare, and readies us for the next one down the pike. But there were already huge problems with the entire variant narrative.
Omicron had no discernible lineage; it seems to have landed fully formed. For it to be a direct descendant of Wuhan, an unfeasible amount of evolution would have to have occurred in an impossibly short time period. Furthermore, natural mutations in viruses always occur randomly and most have no real effect. These types of mutations are known as synonymous. It's the non-synonymous ones that we are interested in, the ones that prove to be impactful, and there is a consistent proportion of one to the other in cases of natural evolution. Not so with Omicron; almost all the mutations are impactful.(20)
This was thought to be evidence that Omicron was also lab-made. But could it not be the result of sloppy work by whoever was responsible for inputting the sequence to the genetic database, some sort of cut-and-paste job, and that Omicron (in the wild) doesn't exist? It's not as if there is definitive proof that any of the other variants actually exist, either. In fact, two Japanese researchers have found the opposite to be true:
“...the official omicron variants ... have just a single synonymous mutation in the gene encoding the spike protein - as compared to 31 to 38 non-synonymous mutations....this makes no sense. Natural evolution would always be expected to create neutral synonymous mutations at a greater rate than non-synonymous mutations that can only persist if, against high odds, they result in a design improvement in the protein they encode.”(21)
The non-existence of Covid and its mutant offspring also makes sense on a practical level; I could never imagine 'them' releasing a dangerous pathogen, for fear that 'they' might also become infected. I felt that the alleged virus was always simply a means to and end, the end being the 'vaccine'. That was where the harm was to be done, where it could be controlled. An infectious pathogen always seemed too much of a risk. I think that logic dictates that the next 'pandemic' will also be a theatrical production.
However, if the evidence that Covid was not a pandemic, but simply a brief interregnum induced by mishandled 'cures' for an imaginary pathogen is credible (whether those cures were intentionally misapplied or otherwise), which it is - given that the data that support that contention are drawn from official publications, the enemy's territory – are we not left with the realization that the Covid conspiracy is even bigger than we thought?
Which, once again, perhaps ought not to be that much of a surprise. Really big lies are often easier to maintain that small ones, simply because most people cannot be persuaded that the state could be that conniving and actively engaged in an attack on public health. These would be the same people who lined up for an experimental gene therapy not once but, in all probability, thrice and who still cannot compute how it is that an infeasible number of their friends and family are now disabled or dead. The state lies big all right and the evidence is that Covid itself is yet another whopper.
Nonetheless, the likelihood is that the bulk of the resistance media will continue down the conventional 'lab leak' rabbit hole for a while longer, content to gorge on a succession of limited hangouts fed to them by the blob. Taking stock and reviewing even the basics is unlikely to be palatable to those who have taken vehement positions which they now wish to defend. There are as many narratives on our side of the fence as there are on the enemy's.
However, a no-pandemic theory isn't really that radical, is it? Most of us didn't believe it at the time or, at minimum, didn't believe the hype about the virus' deadly properties. Should the revelation that the data supports that skepticism (and reinforces our belief in blob mendacity) be an earth shattering surprise? I would think not.
Citations
(1) https://www.zerohedge.com/covid-19/chinese-lab-sequenced-covid-19-weeks-beijing-disclosed-data
(2) https://www.zerohedge.com/geopolitical/science-service-agenda
(3) https://www.thegwpf.org/content/uploads/2023/09/gwpf-open-peer-review-Kelly-et-al-Review-Draft.pdf
(4)

(5) Zachary J Madewell, et al Household Transmission of Sars Cov 2. A systematic Review & Meta Analysis 2020
(7)
(8) Ditto
(12)

(13) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7833340/
(14)
(15) https://dailyexpose.uk/2022/01/26/cwh-discusses-blanket-dnrs-and-litigation-prospects/
(16) https://www.amnesty.org.uk/files/2020-10/Care%20Homes%20Report.pdf
(18) https://www.nytimes.com/article/andrew-cuomo-nursing-home-deaths.html
(19)
(20) https://www.sinobiological.com/
(21) https://zenodo.org/records/8254894
Figure 1
Figure 2 Ditto
Figure 3 Ditto
Figure 4 Ditto
Figure 5 Ditto
Figure 6 Ditto
Figure 7 Ditto