

Say It Ain't So

We've all now heard of mRNA, haven't we? We may not have done two years ago, but the words have been difficult to avoid in the recent past. We may even be confident that we know exactly what it is; some of you almost certainly do. For the rest of us, a small refresher, because it seems to me that we may have been missing something obvious.
“mRNA is the translated form of DNA. mRNA is a fundamental link between what we think of as being the code of life and the actual cell being able to construct a living organism. mRNA is a crucial piece of the fundamental way in which living organisms are created.”(1)
And how does it work, exactly?
“RNA (ribonucleic acid) is a nucleic acid present in all living cells that has structural similarities to DNA. The backbone of both RNA and DNA are made of a phosphate and sugar group. Natural mRNA carries protein information from the DNA in a cell’s nucleus to the cell’s cytoplasm (watery interior), where the protein-making machinery reads the mRNA sequence and translates each three-base codons (i.e. ACG) into its corresponding amino acid to create a protein.”(2)
Crucially, for our purposes, mRNA in the cell's nucleus migrates into the outer cytoplasm, which is where the magic happens. And there the mRNA must remain, as it cannot survive outside the cell. This fact is well established. In any event, as we have seen, it's not supposed to be added to the cytoplasm from outside the cell – it lives within the cell itself. Furthermore, fiddling with Nature and attempting to insert mRNA into the cytoplasm is a daunting task.
“Naked, unformulated mRNA is, however, unable to cross the cell membrane and is susceptible to degradation.”(3)
There is a reason for this. The body, while keen to foster the production of its own, native proteins is far less committed to the prospect of having its cellular factory hijacked by foreign mRNA. Those Big Pharma scientists who are seeking to exploit mRNA technology for profit have had to overcome some significant obstacles:
“Enzymes in the environment and in our bodies are quick to chop mRNA into pieces, making lab experiments difficult and the delivery of mRNA to our cells daunting.”(4)
This is why we have been introduced to another new descriptor – lipid nanoparticles, because
“Fragile mRNA molecules used in the COVID-19 vaccines can’t get into cells on their own. They owe their success to lipid nanoparticles that took decades to refine.”(5)
I take issue with the use of the word “success”, but no matter. In the minds of Bourla (Pfizer), Bancel (Moderna) and others, RNA is cheap to synthesise and, if they could just overcome some of the pesky downsides.
“...for these RNA modalities to reach their full potential, they first need to overcome a billion years of evolutionary defenses that have kept RNAs on the outside of cells from invading the inside of cells. Overcoming the lipid bilayer to deliver RNA into cells has remained the major problem to solve for widespread development of RNA therapeutics, but recent chemistry advances have begun to penetrate this evolutionary armor.
Unlike small-molecule drugs that can slip across the lipid bilayer, the vast majority of mRNA-based therapeutics are too charged and/or too large to enter cells and require a delivery agent.”(6)
The act of plotting to overcome a billion years of evolutionary defenses doesn't seem to have given anyone pause for thought. But that's because they know best, not Mother Nature. And when man's natural defences are standing in the way of the acquisition of mountains of dollars, there's only going to be one outcome. Chesterton's Gate, a principle which holds that nothing should be done away with until the implications are understood, has been ignored; the moral dimension that should be addressed when any decision to override Nature is in the offing has been totally lacking.
Even Ralph Baric of Chapel Hill, North Carolina (a figure with whom we are going to become much more familiar) who, along with Fauci and Peter Daszak of EcoHealth Alliance, forms the high command of the 'vaccine' cult across the pond, was forced to admit that (after decades of attempting to weaponise coronaviruses)
“WIV1-coronavirus (CoV) cluster…may undergo limited transmission in human populations…in vivo attenuation (attenuation means that SARS-CoV-2 becomes extremely weak once inside the human body) suggests additional adaptation is required for epidemic disease.”(7)
To my ear, he sounds a little disappointed. But he wasn't the lipid nano-particles (LNPs) guy. The reason for all the quotations is to hammer home one point – the 'vaccine' needs a delivery agent and that delivery agent is the nano-particles. Without them, the 'vaccine' can't enter the cells. You may have already guessed where I'm going with this. It seems to me that there's an obvious question that hasn't been asked; one that would make any debate about the origins of SARs CoV 2 redundant. If the 'vaccine' can't enter the cell without piggy backing on the back of the LNPs, then how did the virus do so? And how did it become capable of human to human transmission? Because neither of those conditions are common; nor are they simultaneous developments.
The process is known as zoonosis. There are perhaps as many as 1.6 million animal viruses – only 219 of them are known to infect humans, a rate of around 0.01%. So, before we start, we are breathing rarified air.(8)
More precisely;
“...zoonosis requires that human-compatible viral variants pre-exist in the animal reservoir, arising before these viruses have ever even experienced the selective constraints of the human body. For the vast majority of animal viruses in nature, there are just too many protein–protein interactions to master by chance in a random encounter with humans.”(9)
It's complicated, but the gist of it is that it's a two stage process. The virus has to be 'off the shelf', already able to infect human cells and then, once it has gained a foothold, to mutate sufficiently so as to become as transmissible as possible. The virus has to penetrate non specific barriers (such as the skin, stomach acid), then specific barriers (the make-up of the exterior of the human cell, in order to successfully 'dock'), then recruit hundreds of human proteins to replicate it, without encountering a single non matching protein that could scupper the whole deal, even before adaptive immunity kicks in after a few days.
Adaptive immunity helps the host recover, but won't prevent potential spread if viral titers are high enough. If the virus is not well adapted to transmission, inasmuch as it may cause low levels of inflammation for example, it may not spread well or, indeed, at all. If the virus pops up in areas with low population density, it may not spread well either, regardless of its virility. As I hope is clear, an awful lot of ducks have to be in a row for a virus to transfer from animals to humans and then between humans. With regards to specifics
“...it is known that bat coronaviruses require mutations in their surface glycoprotein (spike) in order to use the human ortholog of their receptor, ACE2. But when coronaviruses are sampled from wild bats, a small number of them already encode spike variants compatible with human ACE2. The critical question is, how many additional obstacles (if any) do these viruses need to overcome to replicate themselves in human cells?” (10) (11)
It is known that the surface proteins of human cells, the ones that viruses use to bind them to cells, are among the most likely proteins to change sequence under selection pressure, in order to inhibit the ability of a viral cell to bind. This is probably because of the huge importance of that process; if the viral cell can't bind, it can't hope to infect. This would, in turn, mean that the virus would need to have the exact same pattern of proteins as the cell surface. (12)
The process that is described goes to the heart of the debate as to natural origins for SARs CoV 2. It is clearly entirely possible to take a natural virus that is not off the shelf adapted to humans (because the spike protein is incompatible), change the spike protein for one that is adapted, either because it's been found in the wild or by virtue of lab manipulation, and you have a viable virus.
The furin cleavage site on the SARs CoV 2 spike protein is a major red flag, as they have not be shown to survive in nature in either B type coronaviruses or in influenza; only in the laboratory or via genetic engineering.
“In addition to the possibility of obtaining a furin cleavage site through natural recombination in a secondary host or through serial passage... one could have been spliced directly into the novel coronavirus's backbone in a laboratory using classic recombinant DNA technology that has been available for nearly 20 years. This allows for the removal of the restriction site junctions that are the telltale sign of direct genetic manipulation...so although the entire spike-protein RBD was not assembled from scratch, it is certainly plausible that the 12-nucleotide-long furin cleavage site could have been spliced directly into SARS-CoV-2.”(13)
I appreciate that I haven't chosen to dwell on the possibility that this disease arose in Nature. No host has been found (the disease has this is common with the original SARS and with MERS) and the possibility of that happening is vanishingly small. There is much further evidence that undermines the nature origin argument, which I will come onto later. At present though, as Master Baric and others have noted, the problem of getting the mRNA into human cells remains. It's not enough to have an enhanced furin cleavage site – the virus will still have to dupe the immune system, overcome a billion years of evolution and pierce the lipid bilayer. And then, somehow, work out how to infect others.
So, it's time for a theory; or, more accurately, a working hypothesis, which will necessarily cleave to the Holmesian advice to eliminate the impossible and treat what remains as the truth. We know several important facts already – mRNA, whether real or synthetic, needs a helping hand if it is to infect cells. Further, the orthodoxy requires us to believe that the furin cleavage site is of natural origin and that it can survive outside of the laboratory; the first contention is extremely unlikely and the second has never been achieved. In combination, as near to impossible as to make no practical difference. And lastly, somehow or other, the virus' ability to infect a humans and its ability to transfer between humans have seemingly been acquired at pretty much the same time – the two stage process, that is so unusual that only one hundredth of one per cent of viruses manage it at all, has supposedly been reduced to a single stage process.
Therefore, the working hypothesis must be this – the mRNA of the virus itself has been manipulated in a laboratory, probably by editing genetic code onto the backbone of an existing virus, making it able to bind to the outside of human cells. So far, so conventional if one's critical faculties are still in working order. But that isn't going to be enough. The virus still has be able to pierce the lipid bilayer and, so far, the only known method of accomplishing this is to wrap the mRNA in a positively charged LNP. Thus, the argument about laboratory origins is null – it can only have come from a lab. And the odds of it 'leaking' are, I would posit, minimal when other factors are considered. But I digress.
A working hypothesis must be challenged against the evidence, such as it is. So, firstly, is there any evidence that pins down the lab part of the theory and the deployment of LNPs in the virus, as well as in the 'vaccines'? Secondly, what shade would a positive answer to the first question throw on the narrative of waves of disease and infectivity, to name but two factors? And, thirdly, how well will the hypothesis match other observable facts, the ones that are already inconvenient to the official version of the 'pandemic'?
Let's turn once more to the esteemed scientist from Chapel Hill, Ralph Baric. By 2015, he'd been working with coronaviruses for decades. He, Fauci and Daszak are all connected. Baric has been the lucky recipient of a tsunami of funding for at least 15 years - $111,727,634 between 2003 and 2021, with $23,082,450 coming in the last two years of that spell.(14) Daszak is also a taker, for want of a better phrase, although on a more modest scale; $4,402,107 between 2014 and 2022, with over $2,100,000 in the last year, all for gain of function bat coronavirus work.(15) Both Baric and Daszak are also connected to the Wuhan lab via their relationship with the 'batwoman', Shi Zhengli. That's the three of them in the picture below. The arrow points to Baric, Daszak is seated immediately to his left and Shi is the lady in the check jacket four places further to the left. EcoHealth Alliance, Daszak's company, seems to serve as the cut-out for Fauci's NIAID, sending US taxpayer dollars to Wuhan.(16)

Figure 1
Despite the $100 million plus, Baric was coming up, if not empty, then shy of expectations. That was when he wrote the paper that I quoted from earlier, which acknowledged that his coronavirus mRNA viruses were not capable of significant human-to-human transmission, if they were able to transmit at all. But, by the beginning of 2018, Baric appears to have had his moment on the road to Damascus. He submitted a request to DARPA the (Defense Advanced Projects Agency), asking for funding for a proposal. Baric (and Shi) state that
“we will develop recombinant chimeric spike proteins from SARs -CoVs...we will reconstruct and characterise pike trimers...and incorporate them into nanoparticles...”(17)
That sounds familiar. But that wasn't all. He also wanted to manipulate the furin cleavage sites, to enable the mRNA to bind to human cells.
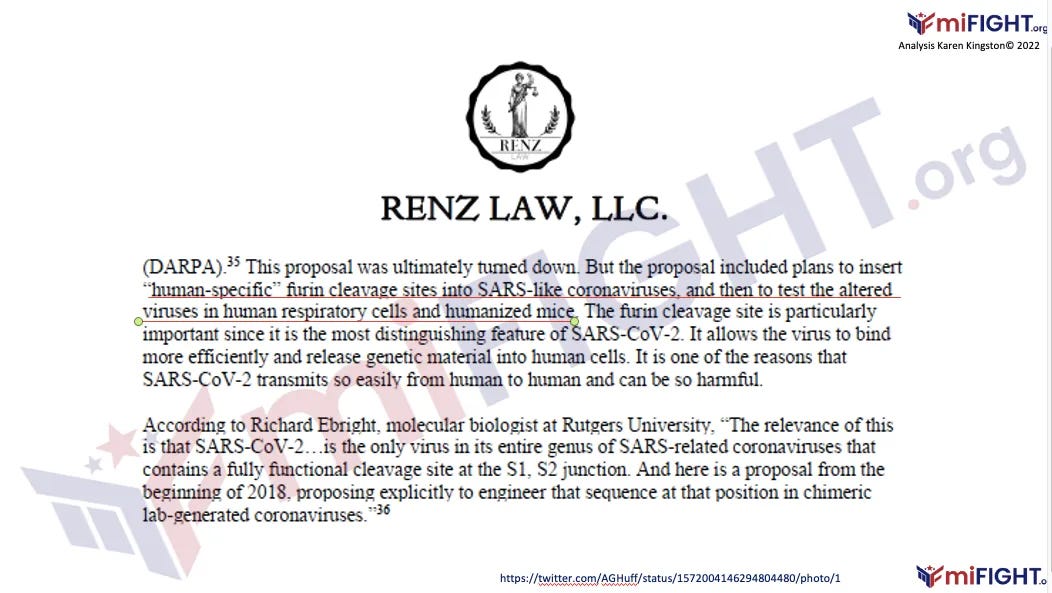
Figure 2
Curiouser and curiouser. And this is the virus, not the 'vaccine'. Well, the spike protein part of it, anyway. These two pieces of engineering – encasing mRNA in lipid nanoparticles and enhancing the binding ability of the spike protein – are precisely what would be required if the virus were to infect human cells. And Baric and Shi were proposing to do just that, even though DARPA wouldn't play ball at that point. It seems likely that the reason for DARPA's reticence was not due to any qualms about the technology, but was instead due to the fact that they were already funding Moderna's mRNA 'vaccine' research through their ADEPT programme, to the tune of $20 million.
“A review of dozens of patent applications found [Moderna] received approximately $20 million from the federal government in grants several years ago and the funds “likely” led to the creation of its vaccine technology. This was used to develop vaccines to combat different viruses, such as Zika and, later, the virus that causes Covid-19.”(18)
Nonetheless, the application is a further, tacit admission that the virus needed to be tinkered with before it would be effective. But does this technology achieve the double whammy that is required for an epidemic? As mentioned earlier, zoonosis is a two stage process; firstly, the virus must infect a human and then it must adapt (within the host) and become capable of transmission between humans. The problem here is that there is scant evidence that there is anything in the mRNA other than spike protein – that goes for the virus as well as the 'vaccine' – although anti-virals such as ivermectin and hydroxychloroquine are effective as early treatments, which would suggest that there was some viral replication taking place. Certainly, the 'vaccines' are only supposed to contain the spike protein, rather than the entire virus genome; Pfizer's FDA approved biological license application makes that perfectly clear.
“COMIRNATY (also referred to as BNT162b2 in this document) contains a nucleosidemodified messenger RNA (mRNA) encoding the viral spike glycoprotein (S) of SARS-CoV-2 that is formulated in lipids including ((4-hydroxybutyl)azanediyl)bis(hexane-6,1- diyl)bis(2-hexyldecanoate), 2-(polyethylene glycol 2000)-N, ,N-ditetradecylacetamide, 1,2- distearoyl-sn-glycero-3-phosphocholine, and cholesterol.”(19)
Even if there was viral material in the lipid nanoparticles that must have been used in the virus, the available research (from Baric himself) shows that transmission between humans is next to impossible. There is no evidence to demonstrate that the conspirators managed to overcome this drawback and plenty to indicate that it wasn't part of the plan. The DARPA application makes no mention of it. Instead, their cunning plan calls for at least four different delivery methods
“...including: 1) transdermally applied nanoparticles; 2) sticky edible gels...;3) aerosolization via prototype sprayers...; and 4) automated sprays triggered by timers and movement detectors...”(20)
None of that indicates that intra human infection is a thing. Which provides us with a puzzle; how did the 'pandemic' get going, then? Well, possibly with the use of these delivery methods – in food, drink or in aerosols, or perhaps a combination of same. Remember, we're just hypothesizing here and then seeing whether it fits the evidence that we do have. Prominent researcher, Karen Kingston, is definite on one point, though:
“The SARS-CoV-2 mRNA virus was never deadly, nor was it contagious. I can’t emphasize this enough, it wasn’t SARS-CoV-2 that caused COVID-19. COVID-19 disease, disabilities and death are the product of Ai bioweapons.”(21)
And, again:
“It's important to note that 'gain of function' viruses are simply mRNA codes....mRNA is a software code. SARS-CoV-2 is not a virus, it's a software code programmed into nanoparticles.”(22)
This is not fanciful. We know that the genetic code that the 'vaccine' is based on is not from a person. The reference from Gen Bank (NC_045512.2) has been confirmed to be artificial, by examination of the database as well as via confirmation from the UK government itself.(23) There are five other entries for SARs-CoV-2 from Wuhan; they are all believed to be genuine, as there are details of the patient and the collection date and time.(24) But it was the synthetic sample that was chosen.
If the virus is not infectious, then here would be a need to keep the 'pandemic' rolling by other means, to prevent people trusting their lying eyes. This required much effort on a number of fronts. An essential tool in this operation was the PCR test. Allegedly, this was phased out in the US over a year ago. The CDC are most unwilling to comment officially, as to the reasons why. All we have is the following:
“In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. Such assays can facilitate continued testing for both influenza and SARS-CoV-2 and can save both time and resources as we head into influenza season.”(25)
Right. So, by a simple process of deduction, that statement is inferring that the existing PCR test doesn't facilitate 'detection and differentiation' of Covid and flu. Not only that, but the head of the CDC is now admitting that the sainted PCR test can stay positive for twelve weeks after infection, anyway.(26) And, of course, the test is intended to be used to confirm a primary diagnosis, not to be used in place of one. The authorities know this well enough. They've chosen to ignore it and hope we don't notice.
Then there is the issue with cycle thresholds. PCR tests amplify viral fragments. These fragments don't need to be alive and the size of them depends on how many amplification cycles are specified. The more cycles, the more white noise. Anything over 30 cycles (at most), is statistically useless and will produce a huge number of false positives. Regrettably, for the duration of this 'pandemic', the cycle rate used by the authorities has been 37 to 40, minimum. It's worth remembering that, at a cycle rate of 35, 97% of PCR tests are false positive.(27) Which was little known and probably still is.
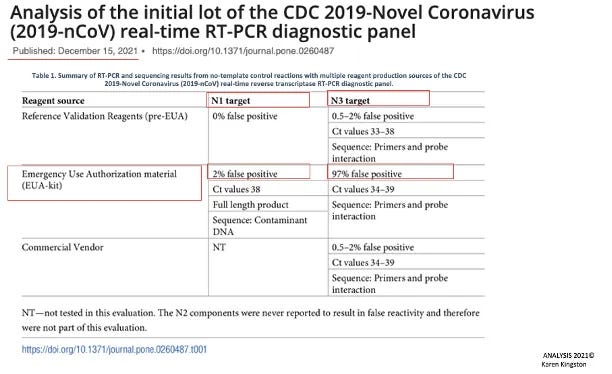
Figure 3
Despite that, by June of last year, testing had gotten out of control.
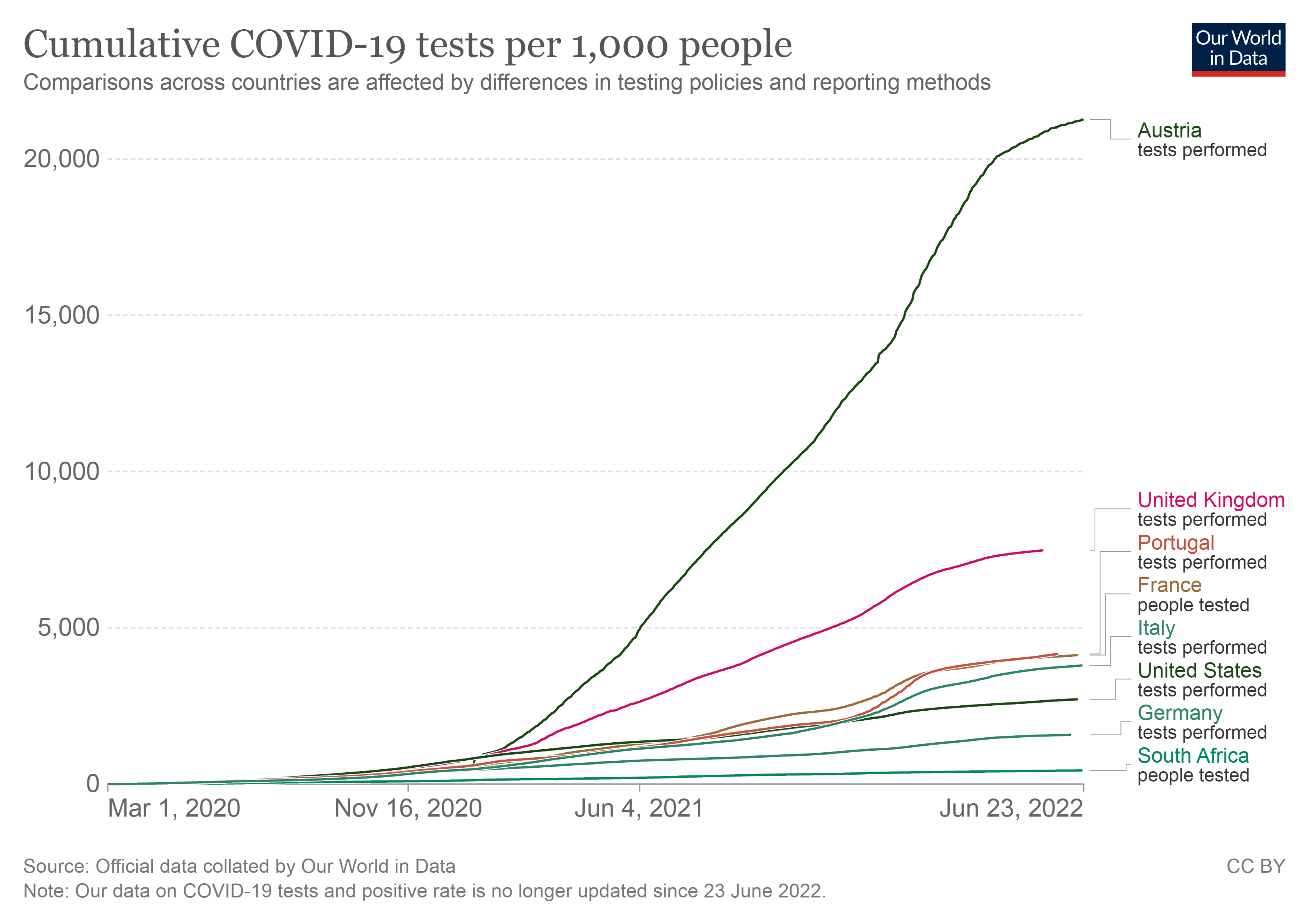
Figure 4
The UK was in the vanguard of the manufactured panic – cumulatively, the population has endured a regime whereby there have been around 7,500 test per 1,000 people. Portugal and France come out at about 4,000 tests per thousand and the United States at 2,600. South Africa managed to dodge this particular bullet, with the equivalent of only 4 in 10 even having a single test, but Austria has been the epicentre of the Covid cult. They tested at a rate of 21,000 for every 1,000 people or 21 for each member of the population. At one point, in June 2021, they were testing over 4,000 people just to get one positive. This is the same country that introduced a government 'vaccine' mandate, with initial fines of €600 (rising to €3,600 every three months) for those who still demonstrated hesitancy.(28)
Given the fact that the PCR test was unable to differentiate between coronavirus and pretty much everything else (including, famously, car oil, papaya and goat's milk, among other random items)(29), but particularly influenza, the next development was unsurprising.
“We've crushed the flu this year. The rate of influenza this year is over 100 times lower than it’s ever been. Why did this happen? It’s obvious: all of the precautions we’re taking to reduce the spread of Covid-19 have worked wonders to prevent the flu as well. In fact, they’ve worked far better for influenza than for the Covid-19 virus.”(30)
So said a gentleman called Steven Salzberg in Forbes magazine. It's a low resolution explanation, but touching nonetheless. However, could it be possible that precautions that don't work for one highly infectious respiratory disease do work for another instead? And, in the light of our new found devotion to vaccines, what effect has the annual flu vaccine had on proceedings, both last season and this?
Well, the US flu season 2020-21 was undoubtedly at a record low. It almost goes without saying, but the following numbers need to be treated with a good deal of skepticism. The Center for Disease Control are the ones providing them and their not particularly well hidden agenda is to persuade the population to get a flu jab, as well as every other inoculation known to man.
In the previous ten seasons, the number of hospitalizations and deaths have trended between estimated totals of 808,000 and 61,000 (2017-18) respectively and 140,000 and 12,000 (2011-12). It can therefore be seen that the difference between a severe season and a mild season is considerable. However, between 10/1/20 and 16/1/21, the CDC recorded only 136 hospitalizations and 292 deaths. That trend has continued, and the current weekly update (end March 2021), shows the hospitalization rate hovering at 0.7 persons per 100,000. This is just a fifth of the rate for 2011-12, an exceptionally mild season.
And it wasn't just the US; during the Southern Hemisphere's winter (our summer), Australia kicked off the season with 14 recorded cases in April (as against 369 the year before) and by June, peak season, that number had declined to zero, where it remained from July to October. Chile recorded 12 cases between April and October, as opposed to 7,000+ the year prior. South Africa had similar results and, globally, it was estimated that by October 2020, recorded cases of flu were down 98% compared to 2019.(31)
Both the CDC and the UK National Health Service stopped counting flu cases in October 2020, which is also a first and difficult to understand as it would surely be important to know what the relationship between the two viruses is. If that had ever been the intention, which it clearly wasn't. October 2020 would have been just prior to an expected flu season and a very strange time to stop counting. The National Health Service were hardly overwhelmed with cases, but perhaps they were too busy testing everyone within eyeshot for Covid. Or, alternatively, there weren't enough sufferers for two diseases and the 'pandemic' was the primary narrative, so flu had to be downplayed.
Interestingly, it's pretty difficult to find charts that provide a global overview of influenza cases from 2019 to 2022/23. This one provides some of the data, but only for the US.
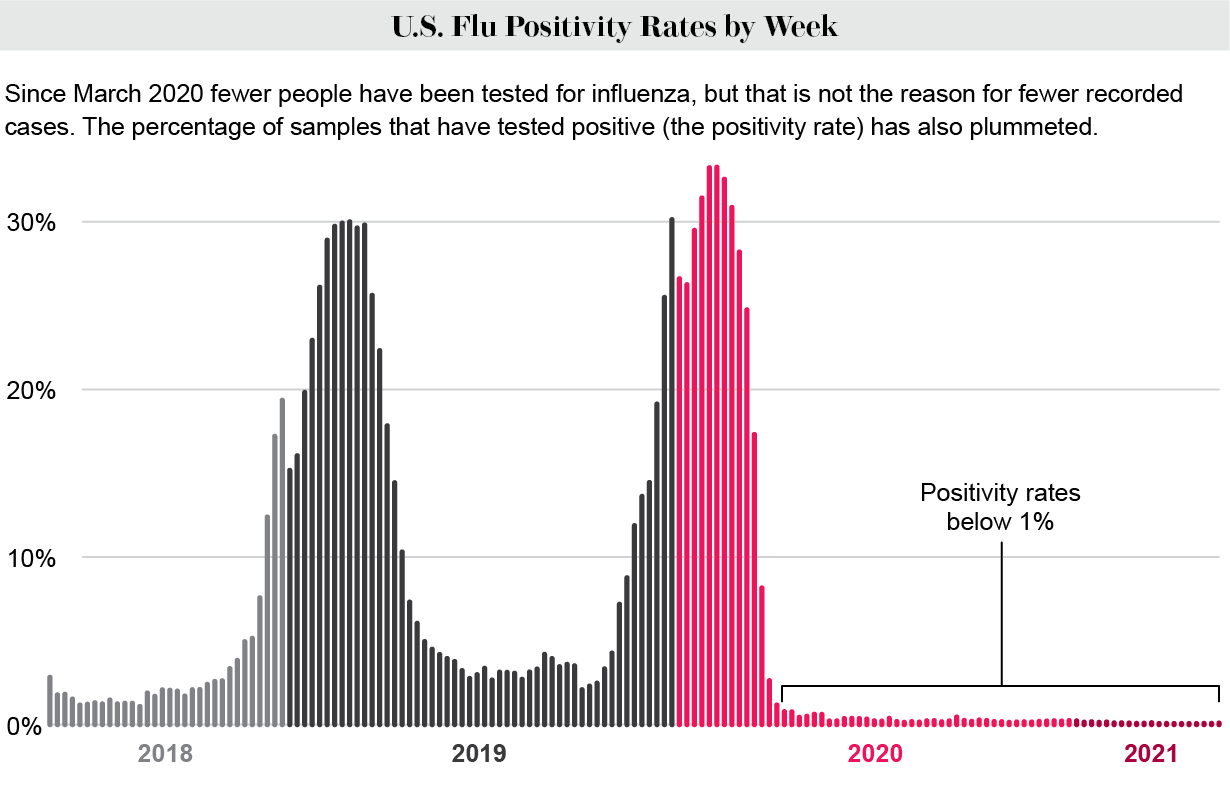
Figure 5
This year, it's not so good.
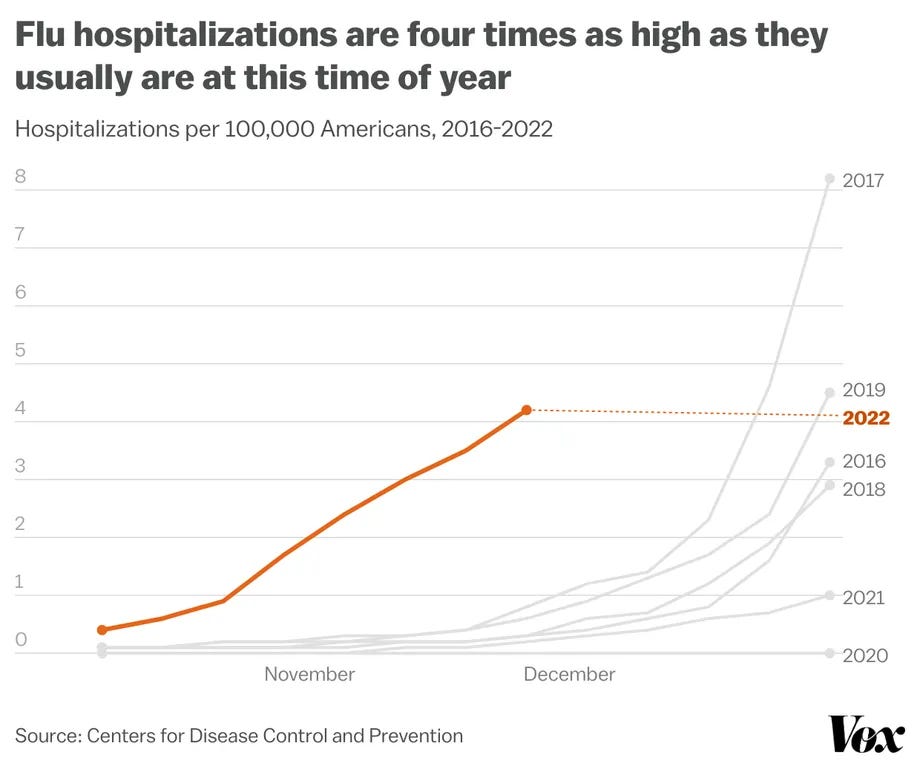
Figure 6
It's not difficult to understand how easily the numbers can be manipulated, when the entire testing and monitoring infrastructure is the same one that is responsible for the Covid response also. It's long been suspected that a number of respiratory complaints have always been lumped in with the flu figures; there's nothing about the entire narrative that is convincing.
There was one other bogeyman that was constantly referenced – asymptomatic spread. The orthodoxy maintained that this was real (even though history and layperson's logic said otherwise) and its purported existence was fodder for the lock-downs and masks mandates. Our working hypothesis dictates that asymptomatic spread would be non-existent and that even symptomatic spread would be difficult, at best. And this is what we find.
A meta analysis, a study of studies, published in December 2020 (and therefore analyzing studies of earlier provenance) found that, among individual households, symptomatic transmission ran at around 18%. Asymptomatic transmission, on the other hand, was pegged at 0.7%.(32) So, roughly one in five symptomatic people passed on the disease, which is a much lower rate than expected and less than 1% of asymptomatic people did same. Or, as per our hypothesis, perhaps infected household members simply ate the same food or breathed the same aerosoled air as the afflicted. This finding was from 54 studies and 77,000 participants and the test subjects were people who were actually living in the same households as the infected, not strangers passing in the street.(33)
Not only that. In the very early days of the 'pandemic' in Wuhan, blood samples were taken from 191 nurses who had been involved in Covid care. None of them had SARs COV 2 antibodies, meaning that none of them had been infected with Covid. That doesn't make sense, if one believes the narrative. If the disease is not efficiently infectious, however, the data are explicable.(34) While we're back in Wuhan allow me to mention that other tests were conducted, this time on nine Covid patients from the food market. The viral genome from each patient was plotted and none of them were a match for any other; all were unique.(35) Once again, this does not compute if we go with the official line – while coronaviruses mutate fairly rapidly, they don't mutate that quickly. If there was some other explanation, which revolved around a release of different strains simultaneously (and there are hundreds of different but similar coronavirus genomes), then we have a possible explanation.
If the virus is not hugely infectious, but is spread by other means, then these studies make sense. They certainly don't provide any succor for existing narratives. It's also possible that the one in five that became infected did not get the virus, but rather picked up an inflammatory condition via the process of shedding. If the lipid nano-particles contained mRNA, or even if they didn't, there wouldn't just be 'vaccine' shedding; there would be viral shedding, too. And the term may well be a cover for a rather more deliberate course of action.
Media such as the Telegraph newspaper in the UK were given their orders as early as March 2020. While talking about the rapidly spreading Wuhan virus, they stated:
“However, if a cure is found, the pace at which it is distributed will be crucial. A range of technologies are being developed to quicken the delivery of vital medicines. One such technology is self-spreading vaccines, whereby the cure spreads through the population in the same way a virus would.”(36)
The New Scientist, in September 2020:
“A cost-effective way to allow a vaccine to “naturally” spread worldwide without the need for developing billions of doses a vaccine to distribute vial injection … involves re-engineering a “benign virus” by adding genetic material from the coronavirus pathogen and infecting large quantities of reservoir populations.
To get a genetically engineered virus to “self-spread” scientists must first directly inoculate a small population intravenously. The small population will then go on to spread the virus aerobically.”(37)
As is usual in these circumstances, tiny objections concerning bioethics and informed consent are swept aside due to the overwhelming emergency facing us. There has been copious anecdotal evidence that shedding is an issue with the Covid 'vaccines', although it can't be the virus itself that is expressed, but rather the spike protein or some other material. In the initial stages after 'vaccination', when the body is a spike protein factory and there are billions of them circulating, it is entirely possible that they can be secreted through skin, bodily fluid and even aerosols.
As far as we know, we have been dealing with what we might term unintentionally shedding 'vaccines', if we were inclined to give the drug companies the benefit of the doubt; but given what we know about Pfizer and the like, that is a risky approach. Especially when those same companies have been doing research on vaccines that shed by design. Naturally, the initial justification will be to experiment in animals, by inserting a small piece of genetic material into a virus that already spreads within the animal community. Apparently, this has already been done in rabbits.
A self spreading vaccine would have a much wider spread than one which is injected into a single arm and the more the replication, the more the chance of mutation and immune escape.(38) Naturally, scientists will think they can find a way around this, because they believe that they can manipulate nature to their own ends, without repercussions. In that spirit, they are already trying to run before they can walk and proposing a version that will 'combat Covid 19'.(39) This is despite the fact that there have been no long term trials, in animals let alone humans, and even the known knowns are potentially catastrophic, in terms of mutation, and therefore having exactly the opposite effect to the one desired; and that's without the unknowns which should become apparent during trials. But quibbles such as these have had no effect on proceedings so far.
And how could such a thing ever be recalled, when its very nature mitigates against it? Once it's out there, it's out there for good and there is nothing that can be done, which makes the need for comprehensive research even more vital. Bear in mind also that there will likely be no redress. Vaccine manufacturers are generally exempt from liability, remember? I don't know whether these 'vaccines' are designed to self spread. But if our overlords were dissatisfied with the rate of take-up or if they calculated at the outset that they would be unable to persuade every citizen to get jabbed, can you see them resorting to a self spreading 'vaccine'? I certainly can.
Are there any other factors that we can point to, which would provide an alternative explanation for the apparent initial deadliness of the virus and the alleged spate of excess deaths? Yes, there are. The hospital and care home protocols were deeply suspect at the time and appear to be even more homicidal in retrospect. It seems clear that 2020 was a year when governments were very keen to ensure that a lot of vulnerable people died, hence the need to flood nursing home with Covid patients, to offer close to $100,000 a pop for a Covid ventilator death and to deny people early treatment that would have saved their lives. By contrast, 2021 was sold to us as the year when the 'vaccines' eliminate the 'pandemic'.
Still, at least hospitals are continuing to rake in federal money for treating 'Covid' patients. A patient that tests positive in a US hospital, whatever the reason for their admittance, automatically becomes a cash cow. Leaving becomes their major problem, as the administrators that run hospital trusts do so for profit and the government has made the internment of a Covid patient very profitable indeed.
There are payments for testing, admittance, treatment with Remdesivir, for every patient on a ventilator and for every Covid death. It is estimated that the full set is worth nearly six figures. I don't know exactly what justification the federal government used at the outset, but I assume it was danger money or similar, an incentive to fearful medical staff to treat the dangerously unclean. It really doesn't take the brains of an archbishop to see that, even at the best of times, that amount of money represents a serious temptation. When it is offered at the same time that hospitals are floundering and going bankrupt due to staff shortages and a lack of income from elective surgery, the net effect is that there is no incentive for hospitals to treat patients with known, effective medications and discharge them swiftly. In fact, the opposite is true. So, once again, are we to believe that this consequence is unintended?
However, the vastly inflated numbers and copious witness testimony indicate that rapacious hospital boards have plundered the riches on offer from the federal government, while abrogating the basic human rights of their patients. They have been assisted in this endeavor by the guidance provided to them by the Center for Medicare and Medicaid,(40) who took it upon themselves to issue blanket waivers (retrospectively to March 1st 2020, just in case some had already jumped the gun). The forty four page document reads like a charter to obviate rights and legitimise abuse. For instance:
“CMS is waiving the requirements at sections....., which require hospitals and CAHs to provide information about their advance directive policies to patients. CMS is waiving this requirement to allow staff to more efficiently deliver care to a larger number of patients.”(41)
So, no longer a requirement to inform the patient about the care plan envisioned for them. This is so far outside the bounds of informed consent as to be over the horizon. It is astonishing that CMS felt they had the right to do these things and profoundly disturbing that they were confident enough to commit them to paper. It illustrates a health care system that is out of control, where the patient's autonomy no longer matters.
Other trends have developed; hospitals went public with their intention to refuse treatment to the 'unvaccinated'. They are already sending these reprobates home from hospital, having denied them quality care and early treatment. This may well be a blessing in disguise, as reports state that around 80% of those enduring the double whammy of Remdesivir and a ventilator (plus a sedative) die in the ICU. These practices, in combination with the vilification of early treatments, were guaranteed to provide bad outcomes. The standard of care for the elderly in care homes was similarly appalling.
The UK government blotted its copybook from day one, but the way that they treated the elderly and vulnerable was nothing short of criminal. This was reflected in the way that the state and the NHS, those paragons of virtue, dealt with treatment of nursing home residents, both in hospitals and in the care homes themselves. Do Not Resuscitate (DNR) notices were one of the mechanisms by which the disabled community and the elderly were culled; that is not a statement that cannot be backed up by the facts.
DNR notices can only be stipulated by the patient or patient's rep. This is accepted practice (42) ever since their introduction, although the NHS had to be reminded of their duties in 2014, when the principle was reiterated via judicial review. This is not difficult stuff; the patient's interests must be represented before any notice may be created. There are no exceptions. These are rights that are preserved in a democracy. Judicial review is one of the ways in which those rights are confirmed. And what happened in 2020, a mere six years later?
The full horror is yet to be revealed but it is known that, between 17th March and 21st December 2020, at least 508 people in adult care facilities had DNR decisions made about them without agreement.(43) We know that the NHS asked care homes to implement blanket DNRs on all their patients and that around 10% of care homes did so – again without agreement.(44) At the same time, the National Institute for Health and Care Excellence (NICE) were issuing guidance (that word, again) which promoted the use of morphine and midazolam, neither of which is an anti-viral and both of which are sedatives.(45)
“Between 2 March and 12 June 2020, 18,562 residents of care homes in England died with COVID-19, including 18,168 people aged 65 and over, representing almost 40% of all deaths involving COVID-19 in England during this period. Of these deaths, 13,844 (76%) happened in care homes themselves; nearly all of the remainder occurred in a hospital. During the same period, 28,186 “excess deaths” were recorded in care homes in England, representing a 46% increase compared with the same period in previous years. These excess deaths likely include undiagnosed COVID-19 deaths, and underscore the broader impact of the pandemic on older people in care homes.”(46)
That's the official version, anyway. The dramatic drop in the level of care, leaving residents vulnerable to all manner of respiratory diseases, and the sudden indifference to the value of a life are much more likely to have been major contributing factors. The vulnerable and elderly, the obvious at-risk category, were clearly not shielded at all and the DNR rules were flagrantly abused. There was law, as established by the courts. There was also yet more guidance, which clearly should not have the same import, but which was allowed to supersede legislation, instead. NICE issued guidance early in the 'pandemic', which targetted vulnerable and disabled people. Targeted is the correct word. The document introduced a “frailty” scoring system.
“with the guideline suggesting that those with a score as low as five – those seen as “mildly frail”, who often need help with transportation, heavy housework and medication (nine represents someone who is terminally ill) – might not be considered appropriate for critical care and might be steered towards end-of-life care instead if their condition deteriorated.”(47)
It seems inexplicable; like flipping a switch and transforming carers into Grim Reapers with the power of life and death. But it happened and it probably still is happening. But it fits the hypothesis; the state had to work awfully hard to get the excess death numbers up in that initial phase. If Covid was a readily transmissible disease, there would have been no need to abuse the DNR system. The residents wouldn't have needed the nudge into the afterlife.
There are four further elements worthy of comment. Firstly, ye olde graphene oxide. The LNP has four ingredients; cholesterol, a phospholipid, an ionizable lipid and a PEGylated lipid. Without getting into the weeds too far, the first two are fatty lipids that cells like and the third possesses a positive charge to penetrate the cell. It's the last one that we are interested in.
When tracked via the specific scientific name, typically a combination of words and numbers, the Moderna version of this lipid is made by a company in China called Sinopeg. The patent, also registered in China, clearly references the use of polyethylene glycol (the PEG part) and graphene oxide in coronavirus vaccines.(48)
And Sinopeg list the nano-particles used in Covid 19 vaccines along with an explanation, which is now severely curtailed, but which wasn't prior to the discovery of their role. One of the ingredients of the polyethylene glycol lipids is graphene, which is, apparently, “the thinnest, strongest and stiffest material ...an excellent heat and electric conductor”.(49)
The second is slightly left field, because we don't have the evidence with regard to the virus, but we do with the 'vaccine'. It's the story of the bio-distribution of the 'vaccine' and its ability to target particular organs. The evidence is applicable to the 'virus' too, if we follow our hypothesis, which holds that the mRNA is almost identical and that LNPs are also deployed in the virus.
It had been previously understood, by the medical establishment in general, that the distribution of the spike protein in the human body was limited to the injection site; the jab is usually administered intra-muscularly, into the shoulder. This is false; clinical trials demonstrated a much wider bio-distribution, which can only be via the bloodstream (50); it seems the likes of Pfizer didn't feel the need to correct false impressions.
The bio-distribution of the spike protein, its action and the presence of PEG and graphene all have quantifiable short term adverse effects. The longer term problems, which should have become apparent in clinical trials (once again), can only be guessed at, although in an educated manner. If tobacco is your poison, your lungs are vulnerable. Drinkers risk liver damage. Whilst there are other secondary vulnerabilities, the risks are well understood. But how do we narrow down disease risk with a toxin that spreads throughout the bloodstream, which can cross the blood-brain barrier? Which can seek out individual weaknesses, exploit them, exacerbate them; weaknesses that may not even be known to the individual? How can we understand cause and effect? Well, if we utilize the science that existed prior to January 2020 – apparently, some upstart doctors are insisting that there is some – we would discover that the likely action of the mRNA 'vaccines' spike protein is as follows:
(a) The spike protein (SP) doesn't stay at the injection site, in the intramuscular tissue, but travels around the body through the bloodstream.
(b) The SP will be taken up by the endothelial cells (cells lining the blood vessels), particularly at sites with slow blood flow, such as smaller blood vessels and capillaries.
A FOIA request in Japan for trial data (as at (50) above) showed that, within hours, the spike protein is distributed around the body via the bloodstream. It enters the spleen (from which diseases such as Alzheimers and Parkinsons originate), bone marrow (leukemia), liver, adrenal glands, ovaries, heart, brain, lungs etc. The 'vaccine' is also expressed in breast milk; not the antibodies, the spike protein itself. The virus affects the lungs primarily, but can also affect the heart, kidneys, the brain, the pancreas and other organs in a remarkably similar pattern.(51)
The third element was the sudden emergence of Omicron. There are some virtually insurmountable oddities about Omicron that indicate that yet another gain of function programme has gone rogue. For starters, SARs CoV 2 cannot infect wild type mice – Omicron can. That being the case, for Omicron to be a direct descendant of Wuhan, an unfeasible amount of evolution would have to have occurred in an impossibly short time period. Furthermore, natural mutations in viruses always occur randomly; most have no real effect.
These types of mutations are known as synonymous. It's the non-synonymous ones that we are interested in, the ones that prove to be impactful, and there is a consistent proportion of one to the other in cases of natural evolution. Not so with Omicron; almost all the mutations are impactful.(52) This outcome must logically be one arrived at via manipulation. There are also no intermediate versions of it, no discernable lineage. It seems to have landed fully formed, with no recent ancestors.(53)
All of this points to the overwhelming probability that Omicron is another manufactured virus, not a variant of the Wuhan strain. But how could this have been accomplished and who could be responsible? And what would be the purpose of releasing a variant that also infects animals? Well, it probably won't surprise you to learn that, far from being chastened by the hue and cry over gain of function research and its probable role in the 'pandemic', scientists have been further manipulating Covid itself to make it capable of infecting mice as well. They aren't hiding it – our old friend Ralph Baric and others published a scientific paper in Nature magazine, detailing the method by which they accomplished it.(54)
It's difficult to credit the arrogance. Baric's project is, in microcosm, the perfect example of how gain of function has gone far beyond any justifiable remit. Why would it be necessary (or even useful) to adapt a virus so that it infects mice, in order that a counter-measure might be created, when the chances of such an event happening in nature are extremely slim to none and, in any event, many years away? It is far from certain that, even if man had the same close interaction with mice that he does with cats and dogs, any mutations would ever cause the disease to jump from one species to the other and yet we find scientists pursuing this line of research anyway. Surely, there must be more pressing matters to attend to.
But no, apparently not, despite the fact that there is no moral justification for carrying out risky research for no discernable benefit. Baric did it anyway and then patented the methodology.(55) So, the timeline is a) a paper published in August 2020, b) Omicron discovered November/December 2020 and c), patent filed February 2021. Baric's virus is also engineered to be particularly pathogenic to aged mice.
To be clear, this virus (SARs CoV 2MA) and Omicron are not identical, but both are mouse adapted and computer designed.(56) The timing is also persuasive. Could it be that Baric also designed Omicron, using the same methods? It's not possible to be definitive, but it would be a hell of a coincidence if he or his colleagues didn't. And the purpose? Well, one outcome, whether by design or otherwise, has already landed as authorities are making much of their belief that wild deer are also capable of being infected with Covid. Wouldn't it be convenient if there was a consensus that gave the cabal the opportunity to further target meat consumption, a task which they are already engaged with?
And, lastly, we must come to the issue of patents. On January 28th 2000, a patent application (6372224) was filed at the US Patent Office on behalf of Pfizer Inc. New York. It was an application detailing the genomic sequence of a spike protein targeting canine coronavirus, together with a binding protein, a vaccine and a method of administering the vaccine.
On April 19th 2002, a further patent application was filed (7279327) on behalf of the University of North Carolina at Chapel Hill. One of the applicant names was the infamous Ralph Baric (more on him later). This was for a replication defective coronavirus, targeting the epithelial cells in the lungs. It includes gene sequencing for the ACE receptor, the ACE2 binding domain, the S1 Spike protein and other elements, engineered and synthetically modified in a laboratory.
“This invention relates to a newly isolated human coronavirus. More particularly, it relates to an isolated coronavirus genome, isolated coronavirus proteins, and isolated nucleic acid molecules encoding the same. The disclosure further relates to methods of detecting a severe acute respiratory syndrome-associated coronavirus and compositions comprising immunogenic coronavirus compounds.”(57)
In layman's terms, this was an attempt to patent a naturally occurring coronavirus and the means of its detection. Should there be any future problem with said virus, it would allow the applicants to have patents and control over all elements in the scenario. It shouldn't be possible to patent a naturally occurring substance and there was significant push-back from the patent office until the CDC overrode their decision to reject the patent and pushed it through.
Patent 7776521 couldn't be more explicit:
“Disclosed herein is a newly isolated human coronavirus (SARS-CoV), the causative agent of severe acute respiratory syndrome (SARS). Also provided are the nucleic acid sequence of the SARS-CoV genome and the amino acid sequences of the SARS-CoV open reading frames, as well as methods of using these molecules to detect a SARS-CoV and detect infections therewith. Immune stimulatory compositions are also provided, along with methods of their use.”(58)
Yes, you read that correctly. That is a patent for the SARS coronavirus, the one responsible for the outbreak the previous year. Additionally, further bacterial and viral pathogens were being patented by the NIH, the US Armed Services and others in the autumn of 2001. Around this time, there was an effort to harness coronavirus as a vector with which to distribute the HIV virus – rather as an adenovirus is being used with the J&J and AZ Covid 'vaccines'. And, given the wide scope and variety of substances patented, consideration was seemingly being given to utilizing coronavirus as a bio-weapon, also.
So, all very interesting, but what is the connection to SARs CoV 2. Well, the very first patent, in 1999, appears to be the progenitor to the SARS virus. The CDC is also shown to hold patents that are 89-99% identical to the sequence identified as SARs CoV 2, as well as the PCR test to detect it. US patent 7279327 shows that not only did the ACE Receptor, the ACE2 binding domain, the S1 spike protein and other elements of SARs CoV 2 exist years before 2019, but also that they were engineered and could be synthetically altered by gene sequencing technologies.
And, finally, there are 120 odd patents detailing all the fine grain, specific, scientific detail of the above elements and substances. What sequences are we comparing these patents to? The genomic sequences posted by the Chinese in January 2020. It's worth letting that sink in. It means that the likes of the NIH, CDC, Chapel Hill at the University of North Carolina and Pfizer hold the patents for SARs CoV 2. They've had them for years.
There's more; patent applications by a company subsumed by Pfizer (again) called Sequoia for an anti-viral treatment for coronavirus, patents transferred between parties already named in November 2018 and the patent vital for current vaccine development shared with Moderna by Chapel Hill in November 2019, before the SARs CoV 2 outbreak officially existed.
In March 2019, Moderna started tidying up four patent applications, changing wording (prior to re-application) to specifically refer to a deliberate release of coronavirus. Moderna also started negotiations with the two Canadian companies that owned patents for the lipid nano-particles technologies that their mRNA vaccine would need. It may be a complete coincidence, but minutes of meetings featuring Dr Anthony Fauci (between 2016 and 2019) record his displeasure at the lack of take up of his universal flu vaccines. Take up of vaccines doesn't seem to be a problem currently, does it?
All in all then, what does this mean? Why were these entities engaged in a flurry of patent activity and the research that lies behind them for a disease, coronavirus, that the WHO states is no longer a concern by 2007/8? Some of this is factual, some conjecture.
Factually, SARs CoV 2, the RT PCR test to detect it and all the specific elements of the spike protein are patented. Patents are not awarded for naturally occurring substances. The patents are owned by a number of organisations, governmental and private and include the NIH, CDC, Pfizer and Moderna. The vaccine is a computer simulation of a spike protein sequence that has been known for years. There is nothing novel about SARs CoV 2. There is nothing natural about it, either.
Moderna were maneuvering in 2019. There was some urgency to their actions, which accelerated their progress towards an mRNA vaccine for SARs CoV 2. Supposedly, they based it on the sequences published by the Chinese; because of the 'pandemic', of course. We now know that the Chinese sequences are just copies of genomic sequences that had been patented in the US.
“So the US Intelligence community funded the bioweapon. Peter Daszak made it with some Chinese assistance. Fauci sold the response. And Moderna Patented it before any of that ever happened. And Bill Gates started pushing vaccines and depopulation, two of the results of the bioweapon, 20 years before the pandemic. What are the chances?”(59)
The more scrutiny the narrative is subjected to, the less believable it becomes. And there are some difficult facts to get past – in particular, the fact that is at the root of my working hypothesis. If mRNA cannot enter the human cell without technological assistance in the form of positively charged LNPs, then it must be engineered. It follows that its infectiousness must be suspect, at best. That being the case, how was a 'pandemic' possible? Answer; it wasn't. It had to be manufactured. Other ailments had to be labelled Covid instead. The mortality rates certainly don't support the idea that there was ever a pandemic.
United States Total Deaths
2010 2,468,435
2012 2,543,479
2014 2,626,418
2016 2,744,248
2018 2,839,205
2020 2,851,432 (to 23/12/20)
World Total Deaths (rounded)
2016 58,000,000
2017 58,700,000
2018 58,500,000
2019 58,800,000
2020 58,800,000
“What can be said is that COVID produced a bump of up to about 15% “excess deaths” in a small number of relatively rich, NATO countries, but in world-wide terms produced no extra deaths beyond what would have been expected for 2020. Most of the hard-hit countries were under, and may still be under, the severest forms of “lockdowns” and “social distancing” such as Italy, UK, France, Spain, Portugal, and parts of the US.”(60)
Excess deaths seem to be confined to a smallish group of Western European nations who share certain characteristics; among them, draconian measures involving lock-downs, social isolation and a refusal to contemplate or allow safe, effective treatments with repurposed drugs. Evidence of a disastrous viral epidemic is difficult to spot. And the fact that governments had to resort to bribing hospitals to maim and kill patients, to instructing care homes to let their residents die, to using a test that was wrong far more often than it was right (amongst other actions) tends to suggest that whatever the disease was, it was not infectious.
There are a few extra points worth considering. The pattern of the initial outbreaks – on cruise ships, in Wuhan, New York etc – is evidence that is neither for nor against the hypothesis. A community outbreak would be indistinguishable from a targetted attack via the water supply or food products. Both scenarios would feature people who were in close proximity becoming ill.
Secondly, if the hypothesis is valid, the variants narrative has to be false. If the virus is not infectious, then there are no opportunities for mutation. And, Omicron aside, how do we know that these variants exist? We are, once again, obliged to rely on the serial liars in governments for that information. After all, the ubiquity of Covid's symptoms means that any number of viruses could fit the bill.
And, lastly, there is the issue of the demonisation of anti-virals. Certainly, these treatments were effective at minimizing Covid symptoms and I can see why allowing their use would torpedo the 'pandemic' narrative and undermine efforts to poison us with 'vaccines'. But there may be a little more to it than that. It seems likely that the likes of ivermectin would be effective against other viruses, too; like influenza. They are now combining the 'vaccines' to both in a single shot and there are further billions of dollars at stake for Big Pharma. Nonetheless, the fact that they went to the lengths they did in the Covid era suggests that the initial nanoparticles may well have been programmed to create a viral load. Kingston certainly believes so:
“Based on the documents I read, in my opinion, the most significant difference between the mRNA nanoparticles that caused the pandemic and the mRNA nanoparticles in the COVID-19 vaccines, is that the original COVID-19 mRNA nanoparticles were programmed to produce a virus in the body, a virus that could make you ill or very ill, but it was not infectious.”(61)
And there we have it. A reminder, if any were needed, that we don't actually know a great deal about the virus. We know we can't trust the state to tell us the truth and very little of what we've been fed has been independently verified. However, it seems that both the virus and the 'vaccine' were created in the laboratory. And it also seems that the virus' infectiousness is mythical; shedding, yes. But nothing more. Food for thought.
Citations
(1) https://www.genome.gov/genetics-glossary/RNA-Ribonucleic-Acid
(2) Ditto
(3) https://pubmed.ncbi.nlm.nih.gov/33829677/
(5) https://cen.acs.org/pharmaceuticals/drug-delivery/Without-lipid-shells-mRNA-vaccines/99/i8
(6) https://www.nature.com/articles/nbt.3802
(7) https://www.pnas.org/doi/10.1073/pnas.1517719113
(8) Anthony SJ, Epstein JH, Murray KA, Navarrete-Macias I, Zambrana-Torrelio CM, Solovyov A, et al. A strategy to estimate unknown viral diversity in mammals. MBio. 2013;4: e00598–13. Pmid:24003179
(9) Warren CJ, Sawyer SL (2019) How host genetics dictates successful viralzoonosis. PLoS Biol 17(4): e3000217. https://doi.org/10.1371/ journal.pbio.3000217
(10) Menachery VD, Yount BL, Debbink K, Agnihothram S, Gralinski LE, Plante JA, et al. A SARS-like cluster of circulating bat coronaviruses shows potential for human emergence. Nat Med. 2015;21: 1508–1513. pmid:26552008.
(11) Menachery VD, Yount BL, Sims AC, Debbink K, Agnihothram SS, Gralinski LE, et al. SARS-like WIV1-CoV poised for human emergence. PNAS. 2016;113: 3048–3053. pmid:26976607.
(12) Letko M, Miazgowicz K, McMinn R, Seifert SN, Sola I, Enjuanes L, et al. Adaptive Evolution of MERS-CoV to Species Variation in DPP4. Cell Rep. 2018;24: 1730–1737. pmid:30110630 (13)www.onlinelibrary.wiley.com/doi/full/10.1002/bies.202000091
(14) https://rumble.com/vlfjc9-karen-kingston-interview-august-19-2021.html
(15) https://reporter.nih.gov/search/td_JdaB1cUqDiVS3gQZ02Q/projects
(16) https://nypost.com/2021/06/04/who-is-peter-daszak-exec-who-sent-taxpayer-money-to-wuhan-lab/
(17)
https://www.darpa.mil/
(18) https://expose-news.com/2022/10/15/how-darpa-and-moderna-pioneered-mrna-vaccines/
(19) https://www.fda.gov/media/151733/download
(20)
https://www.darpa.mil/
(21)
(22)
(23) https://www.ncbi.nlm.nih.gov/nuccore/1798174254
(24) https://expose-news.com/2023/01/23/synthetic-pandemic-covid-manmade-vaccines-deadly/
(25) https://www.medpagetoday.com/infectiousdisease/covid19/95922
(26) https://www.bmj.com/content/375/bmj.n2984
(28) https://www.newsweek.com/austria-implement-vaccine-register-fine-unvaccinated-residents-4000-1657843
(30) Steven Salzberg, Forbes Magazine, March 8th 2021
(31) Mail Online, 20/10/2020.
(32) Zachary J Madewell, et al Household Transmission of Sars Cov 2. A systematic Review & Meta Analysis 2020
(34) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7461296/
(35)
(36) https://www.express.co.uk/news/world/1340352/coronavirus-vaccine-covid19-self-spreading-vaccine
(37) https://www.popsci.com/contagious-vaccine-virus
(39) https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf
(40) Ditto
(41) https://www.ahajournals.org/doi/full/10.1161/circulationaha.105.584532
(45) https://dailyexpose.uk/2022/01/26/cwh-discusses-blanket-dnrs-and-litigation-prospects/
(46) https://www.amnesty.org.uk/files/2020-10/Care%20Homes%20Report.pdf
(48) https://patents.google.com/patent/CN112220919A/en
(49) https://www.sinopeg.com/covid-19-vaccine-excipients_c138
(50) https://www.naturalnews.com/files/Pfizer-bio-distribution-confidential-document- translated-to-english.pdf
(51) https://www.medicinenet.com/which_organ_system_is_most_affected_by_covid-19/article.htm
(52) https://www.biorxiv.org/content/10.1101/2021.12.14.472632v1.full.pdf
(54) https://www.nature.com/articles/s41586-020-2708-8?error=cookies_not_supported&code=ccdc1f30-dd1f-4e90-bccb-19a475a9b6b0
(55) https://patents.justia.com/patent/11225508
(56) https://www.nature.com/articles/s41586-020-2708-8?error=cookies_not_supported&code=ccdc1f30-dd1f-4e90-bccb-19a475a9b6b0
(59) https://expose-news.com/2023/01/23/synthetic-pandemic-covid-manmade-vaccines-deadly/
(60) https://coronanews123.wordpress.com/2021/06/09/global-data-shows-no-excess-deaths-worldwide-in-2020
(61)
Figure 2
Figure 3 https://www.nature.com/articles/nbt.3802
Figure 4
https://ourworldindata.org
Figure 5 https://www.scientificamerican.com/article/flu-has-disappeared-worldwide-during-the-covid-pandemic1/