

Smart Or Stupid?

“There was truth and there was untruth, and if you clung to the truth even against the whole world, you were not mad.”– George Orwell 1984
I have a suggestion; please indulge me. Can we assume that if the government suppresses a viable treatment for Covid, that they mean to do so? That if Pfizer's 'vaccine' is found to contain metals, that they were supposed to be there? That if many thousands are already dead by the 'vaccines' and yet they plough on regardless, then there is something else going on? Because it seems to me that some entities get a free pass, enjoy the benefit of the doubt when there is no reason to give it to them; when we would be better off deploying Occam's Razor, or remembering FDR's maxim that there are no coincidences in politics.
When the state screws up (ostensibly), it seems to me that there are four possibilities:
a) They're stupid.
b) They're smart, but they're happy to let us think they are stupid.
c) They're smart, but they are so out of touch that they don't know we think they're stupid.
d) Their definition of what constitutes success is wholly different to ours.
So, at the macro level there are two choices – stupid or smart. At the micro level, a little more focus on which brand of stupid or smart. But whilst detractors, those who can see the many and varied sins of commission and omission, largely bemoan the fact that dumbness seems to reign supreme. It's not often that mainstream commentators dare to ask the question of whether any (or all) of it is intentional.
The 'lab leak' theory is a classic of the genre. If an alternative theory needs to be called for once the natural origins narratives falls apart, an accidental leak from the Wuhan lab is the only possibility that can be countenanced. It seems that it is either impolite or verboten to mention the obvious problem with this narrow focus, which is that if a virus has come from a lab there are actually two ways that could have happened, not one. It could be accidental or deliberate. And yet, the Big Media default position, once they'd been forced to discard the patently unlikely wet market story, was an immediate assumption of incompetence, rather than malfeasance.
The same goes for any criticism of lock-downs – whether it be the certainty of collateral damage to public health or the inevitable financial Armageddon that results from long periods of home isolation. For the state, the game plan is to ignore any awkward questions for as long as possible. But the more interesting response is from the Fourth Estate; everyone, even the conservative commentators, seems to automatically excoriate government for incompetence. There is another explanation; what if they are smart, instead? What if all that has happened is evidence of a successful outcome, not failure? How is it that this possibility is not even considered?
As a working hypothesis, I'm going to assume that governments have as much expertise as I do on all things Covid. I'm aware that that is giving me much more credit than I deserve on the face of it. But if we believe, instead, that they know more than me, then it'll look even worse for them. So, bear with me. Let's further assume that they are averagely smart, averagely competent. They might not be, but there's a lot of government 'experts' and mandarins and they can't all have room temperature IQ's. We might even be entitled to expect them to get things right sometimes, maybe even a majority of times.
Then let's look at how the Establishment has dealt with the seemingly controversial issue of medical treatment for Covid.
Remdesivir
Remdesivir started life as an investigational drug, an antiviral treatment for Ebola virus. Yet since early 2020, it has managed to gain Emergency Use Authorisation (1st May 20220) and then full approval (22nd October, the same year). It has outpaced even the 'vaccine' approval process and is the only drug authorised for the treatment of Covid in the US. It is also authorised in around 50 other countries.
This is also a drug that even the WHO, no friend to patients worldwide, has said has absolutely no effect on the disease. This finding came from the infamous Solidarity trial, primarily set up to trash the reputation of hydroxychloroquine by poisoning patients with overdoses, in order that they might claim that it was too dangerous to use. But Remdesivir also featured and even this corrupt trial could find no benefit.(1)
The two trials referenced by Fauci when he was talking up the efficacy of Remdesivir do not demonstrate that the drug is safe and effective. They show the exact opposite. The first trial, an Ebola study in the Democratic Republic of Congo, ran from November 2018 to August 2019, but was supposed to last a year. Remdesivir was discontinued by the safety board after 53% of patients died in the first eight months and severe side affects, including renal failure, were commonplace.
Clearly, the prognosis isn't rosy for a patient with Ebola, but two other drugs which were also being trialed were much more effective (monoclonal antibody treatments) and were allowed to continue. The key findings, in reality, were that early treatment is the biggest differentiator between survival and death, that single treatment drugs were more efficient than multi shot regimens and that Remdesivir could, in no way, be claimed to be 'safe and effective'.(2)
A notable feature of academic papers dealing with various aspects of Covid 19 is that the abstract, which is the equivalent of an executive summary, is frequently unrepresentative of the actual results. Thus, a false impression is created. The second trial is a case in point. In this particular example, the abstract emphasizes the finding that 68% of the trial group had enhanced oxygen take-up after ten days. What wasn't mentioned was that 60% of the group also had adverse events and that:
“A total of 12 patients (23%) had serious adverse events. The most common serious adverse events — multiple-organ-dysfunction syndrome, septic shock, acute kidney injury, and hypotension — were reported in patients who were receiving invasive ventilation at baseline.”(3)
So, once again, kidney injury and other organ damage were clear side effects of Remdesivir. There was one further trial, an NIAID trial which was still ongoing at the beginning of May 2020 and which allegedly showed that Remdesivir shortened hospital stays by 5 days, from 15 to 10. The trial had been set up to measure reductions in fatalities, but the objective was changed halfway through (presumably because it didn't seem that the original objective would be met), which smacks of cherry picking the evidence that suits a predetermined narrative.(4)
The EUA references the NIAID trial, but the momentum behind Remdesivir had been created by Fauci's advocacy, which had been on the basis of the alleged results from the other two trials. So, what we have are three trials, all of which are deeply flawed. The first where the drug was deemed so dangerous that the trial couldn't even be completed, the second where one in four patients had severe adverse events within days (and which was conducted by the drug company itself) and the third which changed its desired end point when the data didn't looked like it would pass muster.
But, despite all of the above, from that point forward, Remdesivir was part of the recommended standard of care in American hospitals.(5)
“The emergency use authorization allows for remdesivir to be distributed in the U.S. and administered intravenously by health care providers, as appropriate, to treat suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. Severe disease is defined as patients with low blood oxygen levels or needing oxygen therapy or more intensive breathing support such as a mechanical ventilator.”(6)
We are forced to wonder how it can be that a drug that is known to be toxic to humans, that has a non-existent safety record and unproven efficacy in the treatment of Covid, could possibly be approved for use. How could they be that stupid? Unless they are not being stupid at all. Unless there are other reasons for Remdesivir's sudden rise.
In that vein, it may not surprise you to learn that this treatment is not cheap. The maker, Gilead, is forecast to rake in billions more on top the billions they have already accrued since mid 2020. The cost to the end user is $520 a vial ($390 if the patient is on Medicaid) and there are generally six vials per treatment, although a long treatment course would cost $5,720 per patient. It would be indelicate to accuse them of price gouging, but they have a monopoly and the drug costs $9 a vial to produce.(7) Nice work if you can get it.
Naturally, the company has an entirely plausible explanation for this huge discrepancy. On the basis of the NIAID study, allegedly demonstrating that Remdesivir shortens hospital stays, Gilead calculates that the hospitals are saving $12,000 per patient. Which clearly justifies a markup of nearly 6,000%.(8) As it's the only approved in-patient treatment, it is widely used in hospitals across the country, although the actual protocol seems to be more keenly enforced than in the other 50 nations around the globe. The fact that two types of bonus payments are due to the hospital if the drug is administered, undoubtedly sweetens the pill.(9)
Incidentally, and almost certainly not coincidentally, Gilead is engaged with a drug purchasing group known as UNITAID, a part of the UN Global Compact. The UN group says that its aim is to:
“mobilize a global movement of sustainable companies and stakeholders to create the world we want” by supporting companies to “do business responsibly by aligning their strategies and operations with Ten Principles on human rights, labour, environment and anti-corruption; and take strategic actions to advance broader societal goals, such as the UN Sustainable Development Goals, with an emphasis on collaboration and innovation.”(10)
All of which is standard globalist verbiage about Stakeholder Capitalism, a topic for another day. It may not surprise you to learn that the outcomes being prioritized by the UN have not been voted for by anyone, but rather chosen by our betters. It's sometimes instructive to discover who the interested parties are; in this case, they include Soros, Gates, the Clintons and the WHO, all globally notorious for not having our best interests at heart.
I digress. There are, obviously, one or two problems with Remdesivir. These are exacerbated when treatment is combined with mechanical ventilators and sedatives. So much so that there is a 35% mortality rate in Covid ICUs after 28 days.(11) In particular, in the live setting in hospitals, there are more indications of acute renal failure and cardiac damage,(12)(13) replicating the results of the few trials conducted. Why would it be expected to be any different?
But, as has also been demonstrated with the 'vaccines', clear evidence of serious adverse events and death (which would be the most serious adverse event of the lot) are not persuasive to the FDA, nor anyone else in the medical hierarchy. 'Safe and effective' are still the watchwords, no matter what the state of the evidence is. So, Remdesivir, despite all the evidence to the contrary, is still being used extensively in emergency rooms across the nation.
Summary
At this point, it's worth taking a step back and getting a feel for why and how events are proceeding in this fashion. Without an EUA, Remdesivir would have had to have followed the usual route; standard safety testing, with no guarantee of FDA approval in the far future. The problems that were apparent prior to approval would have been writ large. The drug itself is problematic and unproven. But the way that the medical system operates aids and abets the damage it causes.
Firstly, Remdesivir is an intravenous treatment taken in several sittings; therefore, the patient must be an inpatient. In practice, this entails waiting for symptoms to become serious enough for the patient to be hospitalized. There is no other drug authorised for outpatients. In the early days of the 'pandemic', the most widely prescribed treatments were hydroxychloroquine and Ivermectin, largely because doctors knew that it had worked with the original SARS in 2002. However, in the US at least (and in the EU and the Commonwealth), the moment that Remdesivir was given an EUA, the die was cast.
There are reason for this. For one, the health care system in the US can only be described as shamefully inadequate:
“Obamacare, as constructed, attempted to fix a dysfunctional health care payment system by creating an even more complicated system on top of it, filled with subsidies, coverage mandates, and other artificial government incentives. But its result has been a system that plucked Americans out of coverage they like and forced them to pay more for less.”(14)
Quite how mandating that every American has insurance coverage and fining them if they don't is the answer to anything is not dwelt upon. But there's more.
For example, the extent to which hospitals have established control over medical practices in the US is astounding. Between July 2012 and January 2018, the percentage of hospital employed physicians went up by 70%. Private medical practices have been hoovered up by hospital trusts with the same rapidity as Bill Gates has become a farmer. Over the same five and a half year period, the number of physician practices owned by hospitals went from 35,700 to over 80,000. This is merely the continuation of a trend which began in the late 1980s, where hospitals, insurance companies and other conglomerates getting in on the act.(15)
These entities aren't run by physicians; they're run by bureaucrats, hospital trusts and finance types. Their primary duty, as they see it, is to run a successful business, as defined by the bottom line. The CDC, the NIH or the WHO provide top cover and recommend guidelines and treatments. The insurance companies then institutionalize that advice. The trusts sign agreements with Medicare, Medicaid and insurance companies. They have agreements to promote certain drugs, inevitably at the expense of others. They hold the employment fate of all their employees in their hands and threaten doctors who don't toe the line with termination.
By this method, health care is, effectively, federalized. And it isn't hard to see how profit might interfere with best practice. In fact, it would be a miracle if it didn't. It's the cart driving the horse, an intrusion of a third party into the doctor client relationship.
“It's no secret that over the past several years, America has been experiencing a seismic shift in the way health care is delivered. From government insurance mandates and changes to health insurance design to new reporting requirements, escalating costs and the rise of urgent care clinics, the health care picture has shifted dramatically. And it seems the independent family medicine practitioner is getting squeezed as a result.”(16)
This, of course, is the methodology of Big Government, the Left's panacea to cure all ills. Mandates, regulation, centralization, reporting requirements, 'guidelines'....the usual mantra. And, as always, the result is less choice, less freedom of action and more cost. For independents, who lack the bargaining power of large hospitals, insurance payouts have remained static for several years, even as costs rise. As the state is doing with the First and Second Amendments, so it is here. They won't abolish independents; they'll just regulate them out of existence, if they can.
And in the meantime, the hospitals will keep taking the 20% kickback for prescribing Remdesivir. They don't get penalized for prolonging a patient's stay in hospital. Instead, they get rewarded by the insurance company or the state or federal government; whoever's picking up the tab. And if inpatient care is pretty much the same everywhere, the patient will have little choice but to succumb to the centralized treatment protocols that dominate patient care.
Superficially, it may seem as though 2020 was a bonanza for hospitals, what with a 'pandemic' doing the rounds; but the opposite is true. Hospitals lost hundreds of millions of dollars revenue as they cancelled all but the most urgent procedures and hunkered down to wait things out. The temptation to recoup those losses with hospital stays and sponsored treatments rather than outpatient care with repurposed drugs that cost cents is clear. Immoral, in breach of the Hippocratic Oath, but happening nonetheless.
It's astonishing that the first set of treatment guidelines for Covid patients didn't exist until 8th October 2020 and were published by the National Institute for Health (NIH). No medical societies had bothered to issue advice for nine months at that point, whilst the stage was being set. Predictably, the guidance was that patients were to stay at home and be sick in private until they became unwell enough to come to hospital. Crucially, unwell enough was defined as having difficulty breathing. The hospital would, at some point, provide oxygen and a considerable number of patients would find themselves ventilated and on both a sedative (often Midazolam) and Remdesivir.
By this time, 12-14 days would have passed and any virus still left in the patient would be in sharp decline; either that or gone entirely. The lung problems that present in severe Covid patients are to do with the damage the spike protein causes, not the virus. Micro clotting and inflammation are the enemy at this point in the illness and Remdesivir is of almost no value. Forced oxygen exchange via a mechanical ventilator further damaged lungs that are already compromised.
This, of course, assumes that the original disease was actually Covid. The symptoms ascribed to the virus overlap comprehensively with other coronaviruses, with influenza and with pneumonia, both viral and bacterial. Further, it's not just patients who present with 'Covid' symptoms who find themselves in quarantined ICU. It's also anyone that comes to the hospital with any ailment who then tests positive on a PCR test, with the cycle rate set at 35 to 40. It's worth remembering that, at a cycle rate of 35, 97% of PCR tests are false positive.(17)
The following scenarios are, therefore, plausible and almost certainly happening at a hospital near you;
a) Patients who genuinely had Covid, but now don't, being intubated and given a sedative, an anti viral and forced oxygen which, in combination, worsens the existing condition and also destroys kidney function.
b) Patients with other respiratory diseases which present the same symptoms as Covid but may be bacterial in nature, instead. Unless they are also given a course of antibiotics (some are), anti viral treatment will present no benefits and their disease will worsen.
c) Patients who were at the hospital for something else but who tested 'positive', despite having no symptoms. They are then isolated in the Covid ward, in among people who are genuinely ill and left to take their chances.
There are a couple of other treatments available under CDC guidelines.
Convalescent plasma
Convalescent plasma is taken from donors who have recovered from Covid and contains antibodies that may help suppress the virus. This is another treatment which has been authorised under an EUA, albeit under strict conditions.(18) The authorization, dating from August 2020 has been twice modified and can now only be used on inpatients who are hospitalized with early Covid (when the system is set up to ensure nobody gets early treatment) or hospitalized and suffering from impaired immunity.
The latest wording, from April 2021, is unenthusiastic, using 'neither for nor against' language. And, inasmuch as any medical journal or research paper can be implicitly trusted any more, the New England Medical Journal says that the plasma had no noticeable effect in trials.(19) The narrow scope of the authorization ensures that this treatment cannot be a game changer for many, even if it works.
Regeneron
The only other approved treatment is Regeneron, otherwise known as monoclonal antibodies, aka an investigational antibody cocktail. The antibodies are synthetic and two sets are combined. They work by stimulating an immune response somewhat earlier than would otherwise be the case, thus preventing progression of the disease. They are not a new technology. Coincidentally, Regeneron was also in the Congo trial and demonstrated enough efficacy to be allowed to complete the year long study, unlike Remdesivir.
It has also been granted an EUA (20) and, in what is a consistent theme, it was originally narrowly authorised to be used at the time it would be least effective, for severe cases of already hospitalized patients. It wasn't until April 2021 that authorization was granted to outpatients at high risk of clinical progression (21) and July when the EUA was further expanded to include prophylactic use in those immuno-compromised or otherwise at high risk.(22)
Even now, despite the fact that initial trials have shown a 70% reduction in hospitalizations and overall death and that it is a one stop infusion that can be done in a medical center, the existence of this treatments is not widely known. Nor is it widely available as it is grown in live cells and is therefore difficult to mass produce rapidly. As such, it is a minimal threat to the overall treatment regime, whose emphasis is on delaying early treatment as much as possible. Plus, the supply is under federal control and those states that misbehave can be punished with reduced deliveries, a fate which recently befell Florida.(23)
These are the treatments, combined with steroids and antibiotics, that you may be offered in a hospital or any facility that is not independently run, plus a large number of those that do not suffer under the yoke of hospital boards, but only feel comfortable following official CDC advice. However, there are also independent doctors who are trying to do their job, rather than simply enrich their trust at the patient's expense. There are also many countries around the world who are using tried and tested repurposed drugs with startling results. Startling, compared to the treatment regime in the Western world; not, however, startling to anybody who is paying attention.
Hydroxychloroquine (HCQ)
HCQ has been a safe and effective anti-parasitic and anti-viral drug since 1955. One might be pardoned for thinking that any severe adverse events may have become known by now. The US has 63 million shots in a Washington DC Federal Emergency Management Agency (FEMA) warehouse.(24)
The story of HCQ and Covid is a revealing one. It was prescribed by doctors from the start of the 'pandemic', as it was known to be effective against coronaviruses. It didn't take long for things to change. The first indication that things were not on the level was when the FDA issued an EUA for HCQ in spring 2020. EUAs are not necessary or appropriate with drugs that are already authorised. How is it possible to issue an EUA for a drug that has already been in use for 65 years? It is clear that the agency wanted to insinuate itself into a process in order to control it and it did so by removing doctors' ability to prescribe off label drugs. It was a blatant overreach and yet medical boards and societies said nothing when this unprecedented action was taken.
The EUA restricted its use to inpatients, immediately curtailing its use in early treatment which is when it works best. It also allowed states to impose their own restrictions, a tactic the Blue states (in particular) were keen to exploit.(25)(26) It was a completely transparent attempt to diminish the effectiveness of a treatment that was saving lives; but there were other plans afoot, the better to curtail its prescription.
The NIH had set up a large human trial to test the efficacy of HCQ and azithromycin (AZ) which was all set to launch. Then, fatefully, a paper appeared in the Lancet (probably the world's premier medical journal), which purported to show that HCQ, if used as a treatment for Covid, carried with it an increased risk of death. The study was allegedly reflecting the results of a clinical trial with 96,000 enrolled subjects. It was, however, entirely fictitious and the paper was retracted within a fortnight.(27) But it's job was done by then. It gave the NIH grounds to cancel the trial (28) and for the EUA to be withdrawn. Months later, newspapers were still writing stories condemning HCQ and quoting the study as a source.
Next came the infamous Solidarity/Recovery trials which overdosed patients with at least three times the appropriate dose, killing several hundreds in the process. HCQ was not even intended to be a factor in the WHO sponsored trials, until several countries requested its inclusion.(29) No matter. A way was found to discredit it; the fatalities were clearly viewed as necessary collateral damage.
These events enabled the FDA to state that HCQ should not be used in the treatment of Covid; the medical boards and the pharmacy boards then parrot these guidelines. For a while, there was the ludicrous situation in which a doctor would prescribe HCQ and the pharmacy would then refuse to fill the prescription for the patient.
There have been other events that look to be more than coincidental. In December 2020, the world's second largest manufacturing facility for HCQ precursors burnt to the ground in Taiwan.(30) This after an explosion. Amazingly, two other fires followed at other manufacturing facilities, in the US and Mexico.(31) After explosions. As the old saying goes; if it walks like a duck and talks like a duck, it's a duck.
The problem, as far as the narrative goes, is that in reality HCQ is highly effective at treating Covid and there are any number of studies showing just that.(32)(33)(34)(35)(36)(37)(38) And, in those countries not in thrall to supranational organisations that do not have their best interests at heart, treatment with HCQ has been a resounding success.
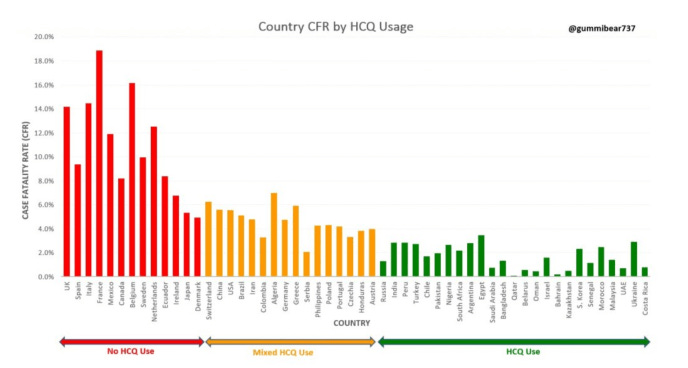
Figure 1: Hydroxychloroquine use in selected countries
Nonetheless, despite all the evidence to demonstrate its safety and effectiveness, there has been a massive, concerted campaign to undermine the drug, as part of a wider effort to ensure that there was no approved (or authorised) early treatment option.
Ivermectin
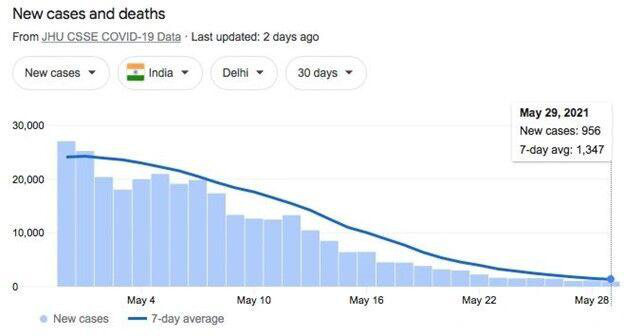
Figure 2: Ivermectin use in India
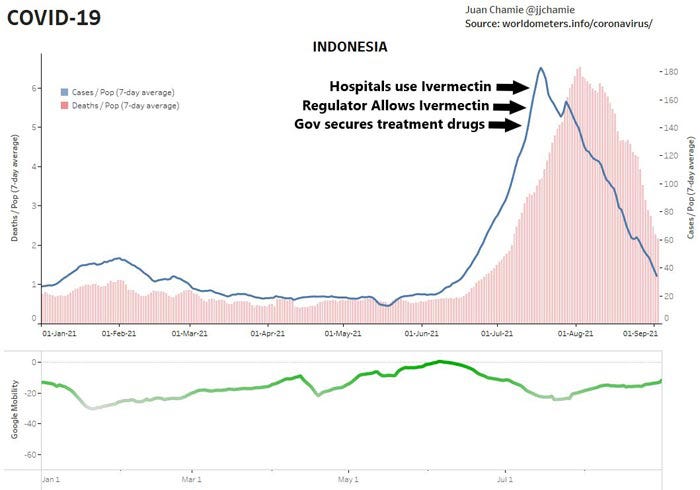
Figure 3: Ivermectin use in Indonesia
With evidence like this, Ivermectin might be expected to be a go-to treatment worldwide. Unlike HCQ, which works best when administered in the early stages of the disease, Ivermectin works on both in and outpatients. It's also effective as a prophylactic and is used as such across large swathes of Africa, where it prevents outbreaks of parasitic diseases. It is known to also have anti viral and anti inflammatory properties and is proven to be around 86% effective in reducing symptoms when used preventively(39). Additionally, it has been shown to kill 99.8% of Covid within 48 hours, all from a single dose.(40) Twenty seven clinical trials have demonstrated efficacy and it has been shown to reduce the damage to internal organs, thus reducing hospital admissions. It also reduces transmission.(41)
Given its qualities, and the fact there is no history of serious side effects, one might expect it to be authorised by the FDA. It is but, once again, the FDA has intervened in ways that are not permitted. Treatment options are for doctors to decide on, but the agency has issued directives stating that Ivermectin isn't approved for use in treating any viral illness. It's not authorized for use to treat COVID-19 within the European Union, either. After reviewing the evidence on Ivermectin, the European Medical Agency (EMA) said that "the available data do not support its use for COVID-19 outside well-designed clinical trials" .(42)
Neither are any clinical trials in prospect and, without clinical trials, Ivermectin will never be prescribed through hospitals and other medical trusts as there will be no guidance statements from on high, providing backup. It will only be independent doctors (who run the risk of losing their medical licenses) who will use this drug for treatment.
There are still pharmacy boards who refuse to fill out prescriptions. There are still letters from medical boards telling doctors not to prescribe it, to let patients get ill enough to be hospitalized so that more lucrative 'treatments' may be utilized instead. And when word leaks out, as it did when Joe Rogan mentioned that he had used it and it was effective, the press launched a co-ordinated effort to characterize it as a horse de-wormer.(43)(44)
Ivermectin, in combination with other drugs and vitamins, is almost certainly the best and safest treatment for Covid, not only at any stage of the illness but even as a prophylactic. But if it was allowed to be used as a viable treatment for Covid, neither Remdesivir nor the 'vaccines' would have been eligible for an EUA, because a key component of the authorization is that no other treatments are available. An additional problem was that HCQ and Ivermectin were already authorised. The solution was to illegitimately assume the power to issue proclamations and authorizations on these treatments anyway and then withdraw permission when the time was right.
There are other treatments, also. In South Africa, where Ivermectin and HCQ have become so politically charged that doctors have been threatened with jail for prescribing them, other protocols have been established, one of which is to wait until day 8 of the disease and then target the virus with steroids, using aspirin and anti inflammatories in combination. Indeed, combinations are the key to treating viruses, as has been found with the likes of HIV and early treatment is absolutely crucial.
It's also worth noting that 40% of drugs are used off label.(45) This is not entirely surprising; as time goes by, more uses become known, complementing the ones for which the drug was designed. But, with Covid, there has been a systemic suppression of early treatment, which has cost hundreds of thousands of lives, whether the treatments are repurposed anti-parasitics or newer technologies such as monoclonal antibodies. The effect has been to allow sick people to get sicker, to suffer more damage. If the authorities can, by their neglect, engineer a situation where the patient ends up in hospital, there is money to be made.
Whistleblowers
Evidence is obviously important; without it, all is opinion and unsupported, at that. It comes in different forms and with differing weight. And, ordinarily, it's wise to draw conclusions when verifiable proof is available. Ordinarily.
But what happens when the evidence is suppressed? When truth tellers are coerced and silenced? When the machine is the entity that is threatened with exposure and it therefore mobilizes to prevent it? And what happens when the machine has the power to manipulate statistics, hide evidence and lie with impunity, safe in the knowledge that nobody with power will call them out? In that scenario, initially at least, whistleblowers are the only source of evidence. And, if momentum builds, there are more of them. That is what is happening in the US right now and it's happening at an increasing rate. This is what they are describing.
Since February 2021, there has been an exponential rise in the number of patients admitted to hospitals with heart attacks, strokes, blood clots, cognitive impairments and other relatively infrequently seen conditions. It seems that hospitals are incurious as to these patients' vaccination status, which is a tad strange as they sufficiently obsessed with Covid to PCR test everyone that comes through the door. Or perhaps they are asked and the answers are deep sixed. It certainly seems likely that they will be questioned as to their ‘vaccination’ status in the future, but only in order to deny treatment to the unjabbed.
In any event, these conditions are suffered by the whole age range, from teenagers up. This, in and of itself, ought to raise eyebrows. It's estimated that, in some major hospitals, around 30% of all admissions are for people with conditions that they shouldn't have. Most are previously healthy, some are older with co-morbidities that are stable and not presently threatening.
It is not possible to be definitive in these cases, merely because doctors and administrators whose job it is to parrot the party line – that the 'vaccines' are safe and effective – are hardly likely to also be the type of person who is questioning as to causation. It ought to be obvious that such a dramatic rise in a suite of conditions that are all documented as potential side effects of the 'vaccines' and which have occurred in lock-step with the 'vaccination' programme is deeply problematic and almost certainly a case of cause and effect. But, cognitive dissonance is a powerful force and it flourishes in conditions where the denial of reality is widespread and pervasive. This seems to be a fair description of most hospitals at the present time.
Normal critical function has been abandoned. There is no other plausible explanation when crash team calls for sudden strokes increase from perhaps two a week to six a night and yet the hierarchy shuts down any questioning as to why. And when incidences of pulmonary embolisms increase from two a week to two a day, also without exciting official comment. It cannot be an epidemic of ignorance, but rather an advanced state of self delusion.
As no connection between injury and vaccine is made or allowed to be contemplated, none of these injuries will be reported as adverse events. That being the case, it is almost certain that the true numbers of injuries is enormous, an order of magnitude higher than the number currently recorded. A recent incident confirmed the truth of this, when an ABC news team used Facebook to fish for stories of people who had died after refusing or delaying the vaccine. Instead, over the course of one weekend, they were inundated with stories of people who had died or suffered serious injury as a result of 'vaccines'; some 39,000 in all. Some individuals knew multiple people who had suffered. There is no reason to think that this is atypical.(46)
If the injuries aren't recorded as adverse events, any subsequent deaths won't be either. But whilst the patients with non fatal adverse event injuries will almost all end up in hospital, those who die as a result of the 'vaccines' won't always have found their way to a care facility. Some will have died elsewhere, suddenly. Either way, a doctor will be required to sign the death certificate but, in the majority of cases, this will be a doctor who will have been recommending the 'vaccine', may even have administered it and will not feel enthused at the prospect of writing 'vaccine death' when to do so would be unpopular with the authorities and compromising to their own reputation.
Other trends are developing; hospitals are going public with their intention to refuse treatment to the unvaccinated. They are already sending these reprobates home from hospital, having denied them quality care and early treatment. This may well be a blessing in disguise, as reports state that around 80% of those enduring the double whammy of Remdesivir and a ventilator die in the ICU.
There are now three categories of what might loosely be termed Covid patients; those who are 'vaccinated' but still have Covid, those 'unvaccinated' and those suffering from 'vaccine' injuries. None of these categories are accurately accounted for; the first two categories because the definitions have been totally corrupted by the CDC (to include, among other things, patients as ‘unvaccinated’ until 14 days after their second shot) and the latter because they are unacknowledged and relatively easy to pass off as unrelated to the vaccines.
The wide variety of possible injuries serves to disguise the common source. If is far easier for the authorities to deny cause and effect when the injuries are spread among a dozen conditions, than it would be if only one injury was predominant, even if the frequency with which previously healthy people are struck down is remarkable enough on its own. And 'vaccinated' people aren't counted as such until 5-8 weeks after they have had their first shot. As a result, the number of allegedly ‘unvaccinated’ patients is greatly inflated, simultaneously reducing the ‘vaccinated’ figure by the same amount; the ‘vaccine’ injured aren't counted at all.
In another development, hospital ‘vaccine’ mandates are now taking effect. It seems that at least 25-30% of care workers will refuse to take the jab. These workers are now in the process of either losing their jobs or resigning. Inevitably, this causes big staff shortages, which then results in closed wards and fewer services. 'Vaccine hesitancy' among hospital staff is a sign of intelligence; after all, nobody is in a better position to connect the dots than they are.
As a direct consequence of their actions, the state and hospital trusts have, between them, managed to contrive a situation where they are experiencing a surge of serious 'vaccine' injury cases, while simultaneously diminishing their capacity to deal with it by sacking staff or losing them to mass resignations. One more arena in crisis, to go with the economy, foreign policy and the southern border. Plus, mandates don't make any sense medically. The same doctors and nurses who were hailed as heroes for dealing with a 'pandemic' for eighteen months, while mostly just wearing an inadequate mask for protection, are now regarded as beyond the pale if they refuse a 'vaccination' that is not only ineffective, but positively dangerous. Once again, as elsewhere, it's not about public health. It's about compliance and, for whatever reason, sticking a needle in every arm.
Conclusion
Hospitals are very dangerous places to be right now. The structure that was created so that we might put safety and wisdom at the heart of medical care has been hijacked. When that happens, the more efficient the system is, the more effective it now is at promoting the bad when previously it promoted the good. This is because, while you would hope that there was room for dissent and discussion within the hierarchy, there often isn't. The structure is efficient but neutral. There are limited checks and balances, or none at all. All that matters is who controls it.
In good times, this inherent weakness is never exposed. But when bad actors are at the tip of the pyramid, it can be catastrophic. The entire edifice comprising the FDA, NIH, CDC, the WHO, the medical associations, hospital trusts and pharmacy bureaus are now working in the cause of evil. A strong word, but what else can it be called? Despite the epic limitations of the VAERS system, there are still over 14,900 deaths recorded that are attributable to the 'vaccines'; a total equivalent to all vaccine deaths for all vaccines for the past thirty years. For context, there are usually around 200 vaccine deaths a year from a total of 500 million shots. And yet, despite all of the above, these entities are all in the business of coercing even more people into getting inoculated.
In this instance, suppression of early treatment was part of the mission. The strengths of the structure now work against the people. The weaknesses are writ large. Now, compliance serves the wrong ends. And, if Big Tech and Big Media are on the same page as Big Pharma and the state, it's very difficult for most people to see what is happening.
It's not just a US phenomenon. The effort to undermine the likes of Ivermectin and hydroxychloroquine has been a global one. In Canada, doctors are told that their licenses will be revoked if they attempt to treat Covid outpatients. In France, doctors are under threat of sanctions or house arrest, in some instances. In Queensland, there is now a law that penalizes any doctor who prescribes HCQ with penalties up to and including a jail sentence of up to six months.(47)
Can you imagine how this could have gone, if the West had done what vast swathes of the rest of the world has done? What would the world look like if we'd suffered their casualty rates, if we'd taken the medications they took both as palliatives and as treatments? Or even just gone the Sweden route and not locked down?
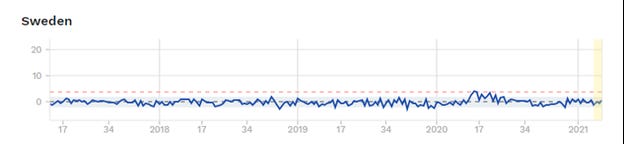
Figure 4: Sweden excess deaths 45-64 years of age
At a conservative estimate, using the micro to illustrate the macro, doctors using these treatments have demonstrated returns of 85% reduction in disease, usually by catching it as early as possible in an outpatient setting. These numbers include those at greater risk of severe disease. If it's not allowed to take hold, it doesn't become severe. If it doesn't become severe, people don't die.
Remember; disease knows no national boundaries. It doesn't do one thing in one place and something different somewhere else. It does something or nothing everywhere. The only factors that can alter those outcomes are treatment and measures such as lock-downs.
To return to the original conundrum, then; which of the four options covers it best? I don't think they are out and out incompetent, because every now and again, even stupid people get things right. But the treatment saga has been one way traffic. Everything governments have done has served one end – to force 'vaccines' upon us all and, through them, 'vaccine' passports and the whole panoply of other control measures that will be introduced on the back of them.
Public health has never been the priority. At no point in medical history have doctors sent people home to wait until the symptoms got worse. Early treatment has always been the gold standard and still is. This cannot be stupidity; it has to be by design.
The necessary sequence of events to bring us from then to now needed to be just so and, mostly, it has been; on occasions it's been difficult to see the seams. At other times, progress has been jarring. For instance, we know that some treatments were already known from the first SARS go-around in 2002 and even before that and these were what were initially prescribed, certainly in the US. Almost immediately though, there was a concerted effort to tarnish these remedies, a course of action that continues even now. Ivermectin is apparently only fit for horses, despite being on the WHO's list of approved medications for decades. The demonization was sudden and a little frantic.
'Vaccines' were the only thing on the mind of the authorities from the end of January 2020. Blinkers were on and, given that decision, there was only going to be one methodology. There was no way that the 'vaccines' would achieve full approval by end 2020; the only possible path to profit lay with an EUA and the conditions for the issuance of one of those include the following:
“FDA may authorize unapproved medical products or unapproved uses of approved medical products to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by CBRN threat agents when certain criteria are met, including there are no adequate, approved, and available alternatives.”(49)
But how to arrive at this destination, how to lay ones paws on the Golden Ticket? To make good on the hundreds of millions of dollars invested in a technology that had thusfar amounted to nothing? How to show that there were no alternative treatments when there clearly were? How about designing a trial of hydroxychloroquine which deliberately overdosed patients? Check. Perhaps by planting a report of an entirely fictitious study in the leading medical journals of the day? Check. Even though it was withdrawn within two weeks, you can still refer to it now and hope no-one notices. Maybe by intimidating the medical establishment (which is now centrally controlled thanks to Obamacare) into prescribing drugs that exacerbate the disease or prevent them from prescribing at all? Check.
Is it just about the money? There are nine new 'vaccine billionaires', including the CEOs of Moderna and BioNTech among others. The other ultra rich elite to have profited from the pandemic include Elon Musk, Bezos, Gates and Zuckerberg. Indeed, the top ten in the list added $488 billion to their wealth between January 2020 and May 2021.(48) The combined wealth of the nine ($19.3 billion) is enough to 'vaccinate' every individual in low wealth country, with change left over. So, transferring public money to the elites is definitely part of it, but it seems that the passports are an essential part of the master plan as well.
Some of the actions taken by the authorities may seem to be so egregious as to be impossible to believe. Surely, if these things happened, you would have heard tell? And there you have the final piece. If nobody is looking, you can pretty much get away with anything. Even if people do look, you can rely on Big Media memory holing the story by ignoring the evidence, or trashing it; which is exactly what they've done repeatedly.
This has been a co-ordinated effort. Not just within jurisdictions, but across national boundaries. It may be the WHO and the USA who are taking the lead for others to follow, or it may be that the likes of Event 201 (a Gates pandemic war game in October 2019) point to prior co-ordination, but Western Europe and the English speaking countries have clearly been in lock-step the entire way.
So, they're not stupid, as in incompetent. The alternative must, therefore, be true instead. They're smart in that they've changed the world in eighteen months and they calculated that we'd let them do it; so far, they've been right. And at the micro level? I don't think they care about whether we know what they're doing. It's likely that there is some group-think, echo chamber ignorance – they didn't see Brexit or Trump coming, after all – but, in all probability, what we think isn't important to them. As long as they can still parrot the same things and enough people do as they are told, it's enough. How many masks? Curfews stop the spread, do they? Booster shots now?
As long as they are not being held to account, they will continue to do what they are doing; the only thing that will alter is the pace of change, which is already quickening. Any effective treatment will become increasingly difficult to source, unless it comes in a needle. They were smart enough not to have made their move until they control all the levers. The only thing they worry about is not what we think, but what we can do to stop them. Their definition of success doesn't look anything like ours. We might want to go back to 2019. They want to turn the clock back to 1984.
Citations
https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1
Mulanga S et al, A Randomised, Controlled Trial of Ebola Virus Disease Therapeutics. N Eng J Med. 2019 Dec 12;381(24):2293-2303.doi:1056/NEJMoa1910993.Epub2019 Nov27. PMID 31774950.
https://www.nejm.org/doi/full/10.1056/NEJMoa2007764?query=featured_home
https://www.jdsupra.com/legalnews/cms-hikes-payment-for-covid-19-19452/
https://www.unglobalcompact.org/what-is-gc/mission
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2768602
https://www.cureus.com/articles/44072-cardiac-adverse-events-with-remdesivir-in-covid-19-infection
https://www.washingtonexaminer.com/conservatives-vindicated-by-obamacares-mounting-failures
https://edition.cnn.com/2020/06/17/health/hydroxychloroquine-national-stockpile/index.html
https://www.ama-assn.org/system/files/2020-04/board-of-pharmacy-covid-19-prescribing.pdf
https://www.nih.gov/news-events/news-releases/nih-halts-clinical-trial-hydroxychloroquine
https://anthraxvaccine.blogspot.com/2020/06/who-trial-using-potentially-fatal.html
https://www.oom2.com/t69648-large-fire-at-magnesium-factory-in-madison-illinois
https://www.sciencedirect.com/science/article/pii/S2052297520300615
https://www.neuromed.it/lidrossiclorochina-riduce-la-mortalita-intraospedaliera-da-covid-19/#
https://link.springer.com/article/10.1007/s11606-020-05983-z
https://www.news-medical.net/news/20200406/Antiparasitic-drug-Ivermectin-kills-coronavirus-in-48-hours.aspx
https://nypost.com/2021/08/22/people-taking-horse-cow-de-wormer-for-supposed-covid-19-treatment/
https://medtruth.com/articles/health-features/off-label-prescriptions/
https://oxfam.org.nz/news-media/media-releases/covid-vaccines-create-9-new-billionaires
Figure 1 https://jeffreydachmd.com/2020/08/hydroxychloroquine-efficacy-against-corona-virus/
Figure 2 https://systems.jhu.edu/tracking-covid-19/
Figure 3 https://worldometers.info/coronavirus/
Figure 4 https://sbhilfe.com/world-news/england-had-more-deaths-than-italy-during-peak-of-covid-19-outbreak/